Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- 10-037.16 Medical Emergency ProceduresDokumen2 halaman10-037.16 Medical Emergency Proceduressuperm0mof6Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Abhinav Kumar Vulisha MBBS Pulmonologist ResumeDokumen6 halamanAbhinav Kumar Vulisha MBBS Pulmonologist ResumeHruday RaajBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- EACMC-C: Profile of Cavite's 154-bed private hospitalDokumen8 halamanEACMC-C: Profile of Cavite's 154-bed private hospitalNicole De AsisBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
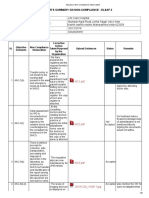
- Assessor Non Compliance ObservationDokumen9 halamanAssessor Non Compliance ObservationSwati BajpaiBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- CV: Anesthesiologist with Experience in EducationDokumen6 halamanCV: Anesthesiologist with Experience in EducationogidoBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- List of Medical Facilities in India: Prepared by British High Commission New DelhiDokumen78 halamanList of Medical Facilities in India: Prepared by British High Commission New DelhiNazim KhanBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- BeneFusion VP5 FP Operator's Manual V2.0 enDokumen114 halamanBeneFusion VP5 FP Operator's Manual V2.0 enherbertamaya0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- SLE5000.Infant Ventilator PDFDokumen8 halamanSLE5000.Infant Ventilator PDFRuban RajBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Sarah Hospital - Joao Filgueiras LimaDokumen35 halamanSarah Hospital - Joao Filgueiras LimaJoao Pedro LacerdaBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Active Amp Passive Voice WktsampKeyDokumen12 halamanActive Amp Passive Voice WktsampKeyGrand OverallBelum ada peringkat
- Dr. Daniel SesslerDokumen2 halamanDr. Daniel SesslerKimAndersonBelum ada peringkat
- Nursing Leadership and ManagementDokumen48 halamanNursing Leadership and ManagementDarl DacdacBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Therapist Driven ProtocolsDokumen3 halamanTherapist Driven ProtocolsPaoly PalmaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Philips V680 Ventilator BrochureDokumen8 halamanPhilips V680 Ventilator BrochureMedSparkBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Técnica Quirúrgica GENESIS II PDFDokumen46 halamanTécnica Quirúrgica GENESIS II PDFsersergioBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Nursing Management Process and Functions Post-TestDokumen5 halamanNursing Management Process and Functions Post-TestArlene CarampelBelum ada peringkat
- History of The Burroughs Wellcome Fund 1955-2005Dokumen100 halamanHistory of The Burroughs Wellcome Fund 1955-2005Russ Campbell100% (1)
- Learning Feedback DiaryDokumen4 halamanLearning Feedback DiaryFerreze AnnBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Caesarean SectionDokumen26 halamanCaesarean SectionMark Bin S. DilangalenBelum ada peringkat
- 04-SOAL LINK-SMK-BAHASA INGGRIS-Kur2006-UTM-1819Dokumen5 halaman04-SOAL LINK-SMK-BAHASA INGGRIS-Kur2006-UTM-1819Juharna HardiantoBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- An Instrument To Determine Orthodontic Bracket Slot Size and Bracket AlignmentDokumen8 halamanAn Instrument To Determine Orthodontic Bracket Slot Size and Bracket AlignmentDawjeeBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- About Pulse OximetryDokumen16 halamanAbout Pulse OximetrySrdjan DimitrijevicBelum ada peringkat
- 4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142Dokumen416 halaman4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142AhmedNadeemBelum ada peringkat
- Accomplishment ReportDokumen8 halamanAccomplishment ReportKevin Fernandez MendioroBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Arnold Palmer Hospital1Dokumen3 halamanArnold Palmer Hospital1Rania Alkarmy100% (1)
- Keys To Nursing Success Chapter 1Dokumen42 halamanKeys To Nursing Success Chapter 1Melissa100% (2)
- Newborn Assessment RedoDokumen8 halamanNewborn Assessment Redoapi-301349934Belum ada peringkat
- Nursing Care Plan For Risk For Compromised Human Dignity NCPDokumen3 halamanNursing Care Plan For Risk For Compromised Human Dignity NCPderic100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- DubaiCare Network List - September 2023Dokumen234 halamanDubaiCare Network List - September 2023mht1Belum ada peringkat
- Mastering Health Economics with OUM Business SchoolDokumen8 halamanMastering Health Economics with OUM Business SchoolMuhammad AliminBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)