Anda mungkin juga menyukai
- Soft SkillsDokumen117 halamanSoft Skillskiran100% (1)
- Salesforce Platform Developer 1Dokumen15 halamanSalesforce Platform Developer 1Kosmic PowerBelum ada peringkat
- Standards of Psychiatric NursingDokumen19 halamanStandards of Psychiatric Nursingamita chaudhari50% (2)
- Fundamentals of Nursing CareDokumen206 halamanFundamentals of Nursing CarePrincess Faye Tiongson ChavezBelum ada peringkat
- Emergency NursingDokumen9 halamanEmergency NursingJamaica WineBelum ada peringkat
- Nurse'S Role in Health AssessmentDokumen24 halamanNurse'S Role in Health AssessmentHAZEL RODA ESTORQUE100% (1)
- DOH Program CertificationDokumen1 halamanDOH Program CertificationMarti Gregorio100% (1)
- Duplex Color Image Reader Unit C1 SMDokumen152 halamanDuplex Color Image Reader Unit C1 SMWatcharapon WiwutBelum ada peringkat
- National Core Competency StandardsDokumen89 halamanNational Core Competency Standardsverna100% (1)
- PSISA Free Practice Exams TestsDokumen2 halamanPSISA Free Practice Exams TestsGoodmanBeguel50% (2)
- Leadership and Management in NursingDokumen5 halamanLeadership and Management in NursingSolsona Natl HS Maananteng100% (1)
- Professional AdjustmentDokumen140 halamanProfessional AdjustmentRaquel M. MendozaBelum ada peringkat
- Assistant Director of Nursing Care: Passbooks Study GuideDari EverandAssistant Director of Nursing Care: Passbooks Study GuideBelum ada peringkat
- Clinical Evaluation Tool 432Dokumen9 halamanClinical Evaluation Tool 432api-470941612100% (1)
- Approvals Management Responsibilities and Setups in AME.BDokumen20 halamanApprovals Management Responsibilities and Setups in AME.BAli LoganBelum ada peringkat
- A Nursing PortfolioDokumen7 halamanA Nursing Portfolioabhi100% (3)
- Fundamentals of Nursing (Midterm Topic 1)Dokumen7 halamanFundamentals of Nursing (Midterm Topic 1)Manuel, Precious Marie B.Belum ada peringkat
- Code of Ethics For NursesDokumen3 halamanCode of Ethics For NursesLady Mae Ramos100% (3)
- Prof. AdjustmentDokumen111 halamanProf. AdjustmentDianne Kate CadioganBelum ada peringkat
- Leadership in Nursing Nursing AdministrationDokumen18 halamanLeadership in Nursing Nursing AdministrationKen Lam100% (1)
- Nursing Leadership and Management: Ma. Christina B. Celdran - Oraa, PHD RN Assistant ProfessorDokumen29 halamanNursing Leadership and Management: Ma. Christina B. Celdran - Oraa, PHD RN Assistant ProfessorTotoh HaidsBelum ada peringkat
- The Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionDari EverandThe Ethic of Care: A Moral Compass for Canadian Nursing Practice - Revised EditionBelum ada peringkat
- Britannia FinalDokumen39 halamanBritannia FinalNitinAgnihotri100% (1)
- A. Teleological Approach or Act of UtilitarianismDokumen13 halamanA. Teleological Approach or Act of UtilitarianismEnrique Babierra100% (1)
- RN Job Description PDFDokumen1 halamanRN Job Description PDFvhon100% (1)
- Nursing StaffingDokumen5 halamanNursing StaffingPeace Andong PerochoBelum ada peringkat
- Hazard Identification Priority Area Checklist Worksafe Gov AuDokumen29 halamanHazard Identification Priority Area Checklist Worksafe Gov Aufh71100% (1)
- NCM 107A-Nursing Leadership and Managemen... (NCM 107A - Nursing Leadership & Management (Lecture) )Dokumen32 halamanNCM 107A-Nursing Leadership and Managemen... (NCM 107A - Nursing Leadership & Management (Lecture) )Jek Dela CruzBelum ada peringkat
- Benner's Stages of Nursing: WHO IS Patricia Benner? Major ConceptDokumen2 halamanBenner's Stages of Nursing: WHO IS Patricia Benner? Major ConceptRhuaine ReyesBelum ada peringkat
- Core Competencies, 2012 NNCCSDokumen23 halamanCore Competencies, 2012 NNCCSJose BernelBelum ada peringkat
- Nursingprocess Assessing 111105015609 Phpapp01Dokumen71 halamanNursingprocess Assessing 111105015609 Phpapp01ALmik HussinBelum ada peringkat
- Home Health CareDokumen2 halamanHome Health CareMisaki AiharaBelum ada peringkat
- Critical Thinking and The Nursing Process LEARNING OUTCOMES AfterDokumen16 halamanCritical Thinking and The Nursing Process LEARNING OUTCOMES Aftertwy113100% (3)
- Critical Thinking and Clinical ReasoningDokumen39 halamanCritical Thinking and Clinical ReasoningAsad KhanBelum ada peringkat
- Complete Drugs StudyDokumen13 halamanComplete Drugs StudyPeace Andong PerochoBelum ada peringkat
- Comparison of the Philippine Nursing Acts of 1991 and 2002Dokumen20 halamanComparison of the Philippine Nursing Acts of 1991 and 2002Joni PurayBelum ada peringkat
- NLM Sas 8Dokumen6 halamanNLM Sas 8Zzimply Tri Sha UmaliBelum ada peringkat
- NNTimes October 09 Issue PDFDokumen72 halamanNNTimes October 09 Issue PDFMonika Joseph0% (2)
- Professional Adjustment and Nursing JurisprudenceDokumen13 halamanProfessional Adjustment and Nursing JurisprudenceFelix Camposano Jr100% (1)
- Nursing Informatics NCM 112: Leslie L. Paguio BSN 3-CDokumen31 halamanNursing Informatics NCM 112: Leslie L. Paguio BSN 3-CLeslie PaguioBelum ada peringkat
- The Problem and Its BackgroundDokumen9 halamanThe Problem and Its BackgroundPeace Andong PerochoBelum ada peringkat
- Record Keeping for Nurses and Midwives: An essential guideDari EverandRecord Keeping for Nurses and Midwives: An essential guideBelum ada peringkat
- Cryptography Seminar - Types, Algorithms & AttacksDokumen18 halamanCryptography Seminar - Types, Algorithms & AttacksHari HaranBelum ada peringkat
- Leading and Managing in NursingDokumen14 halamanLeading and Managing in NursingCharmaine Vergara - Gementiza100% (1)
- CA 2 PalmerDokumen9 halamanCA 2 PalmerEricson SomeraBelum ada peringkat
- NCMB 419 Week 11 CU10Dokumen23 halamanNCMB 419 Week 11 CU10GERALDINE GONZALESBelum ada peringkat
- REPORT - Nursing As A ProfessionDokumen35 halamanREPORT - Nursing As A ProfessionDNS FRDBelum ada peringkat
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersDari EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersBelum ada peringkat
- What Is Next After Passing The Board ExamDokumen6 halamanWhat Is Next After Passing The Board Examtimie_reyesBelum ada peringkat
- STAFFINGDokumen3 halamanSTAFFINGXnikz XnakzBelum ada peringkat
- Nursing Management Process and FunctionsDokumen151 halamanNursing Management Process and FunctionsYum CBelum ada peringkat
- Complementary Alternative ModalitiesDokumen5 halamanComplementary Alternative ModalitiesRinal BaradBelum ada peringkat
- Legal and Ethical Issue in Er PDFDokumen49 halamanLegal and Ethical Issue in Er PDFandaxy09Belum ada peringkat
- Higit Pa Bumuo ng Blog Mag-sign inDokumen7 halamanHigit Pa Bumuo ng Blog Mag-sign inLot RositBelum ada peringkat
- FAQ About IVT TrainingDokumen12 halamanFAQ About IVT TrainingJohanna ChavezBelum ada peringkat
- Board of NursingDokumen3 halamanBoard of NursingLou Cabachete LiveraBelum ada peringkat
- Spiritual and PsychosocialDokumen40 halamanSpiritual and Psychosocialhaddi awanBelum ada peringkat
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDari EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideBelum ada peringkat
- Salem Hospital Nurse Staffing PlanDokumen3 halamanSalem Hospital Nurse Staffing PlanKathlyn Joy EclarinalBelum ada peringkat
- Philippine Nursing LawDokumen2 halamanPhilippine Nursing LawCarlo DadisBelum ada peringkat
- CH 4 - Treatment Settings and Theraputic Programs-Test-Bank-Tank PDFDokumen14 halamanCH 4 - Treatment Settings and Theraputic Programs-Test-Bank-Tank PDFtimBelum ada peringkat
- Funda - Pretest 2Dokumen10 halamanFunda - Pretest 2FreeNursingNotesBelum ada peringkat
- Chapter 1 - Health Care Delivery and Nursing PracticeDokumen4 halamanChapter 1 - Health Care Delivery and Nursing Practicejane amosBelum ada peringkat
- The Icn Code of Ethics For NursesDokumen5 halamanThe Icn Code of Ethics For NursesJazmin Venice Lasala100% (1)
- Leadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Dokumen38 halamanLeadership & Management in Nursing NCLEX Practice Quiz (80 Questions)Mack MakaBelum ada peringkat
- Nsg. EntrepreneurshipDokumen30 halamanNsg. EntrepreneurshipRoseben SomidoBelum ada peringkat
- 4 Developing A Health Education PlanDokumen19 halaman4 Developing A Health Education Planblancher erBelum ada peringkat
- DelegationDokumen24 halamanDelegationJP FernandezBelum ada peringkat
- Nursing Jurisprudence - For UploadDokumen290 halamanNursing Jurisprudence - For UploadBing58Belum ada peringkat
- Registered Professional Nurse: Passbooks Study GuideDari EverandRegistered Professional Nurse: Passbooks Study GuideBelum ada peringkat
- Sergei Vasilievich RachmaninoffDokumen2 halamanSergei Vasilievich RachmaninoffPeace Andong PerochoBelum ada peringkat
- Or ChecklistDokumen2 halamanOr ChecklistPeace Andong PerochoBelum ada peringkat
- Causes of IdwDokumen1 halamanCauses of IdwPeace Andong PerochoBelum ada peringkat
- Review medications, nursing roles, UPH missionDokumen2 halamanReview medications, nursing roles, UPH missionPeace Andong PerochoBelum ada peringkat
- Report EcgDokumen144 halamanReport EcgPeace Andong PerochoBelum ada peringkat
- AbortionDokumen77 halamanAbortionPeace Andong PerochoBelum ada peringkat
- Bone TumorsDokumen22 halamanBone TumorsPeace Andong Perocho100% (1)
- Grade Ii - B S. Y. 2013 - 2014Dokumen2 halamanGrade Ii - B S. Y. 2013 - 2014Peace Andong PerochoBelum ada peringkat
- Review medications, nursing roles, UPH missionDokumen2 halamanReview medications, nursing roles, UPH missionPeace Andong PerochoBelum ada peringkat
- AbortionDokumen77 halamanAbortionPeace Andong PerochoBelum ada peringkat
- Relit For Ate JulieDokumen10 halamanRelit For Ate JuliePeace Andong PerochoBelum ada peringkat
- University of Perpetual Help SystemDokumen2 halamanUniversity of Perpetual Help SystemPeace Andong PerochoBelum ada peringkat
- Angina Pectoris SharinaDokumen3 halamanAngina Pectoris SharinaPeace Andong PerochoBelum ada peringkat
- DrugDokumen3 halamanDrugPeace Andong PerochoBelum ada peringkat
- BiogesicDokumen2 halamanBiogesicianecunarBelum ada peringkat
- Patho ShoDokumen1 halamanPatho ShoPeace Andong PerochoBelum ada peringkat
- RubelinDokumen7 halamanRubelinPeace Andong PerochoBelum ada peringkat
- Potse MindDokumen1 halamanPotse MindPeace Andong PerochoBelum ada peringkat
- Reaction JournalDokumen2 halamanReaction JournalPeace Andong PerochoBelum ada peringkat
- ChancroidDokumen2 halamanChancroidPeace Andong PerochoBelum ada peringkat
- DrugsDokumen2 halamanDrugsPeace Andong PerochoBelum ada peringkat
- Be It Enacted by The Senate and The House of Representatives of The Philippines in Congress AssembledDokumen9 halamanBe It Enacted by The Senate and The House of Representatives of The Philippines in Congress AssembledPeace Andong PerochoBelum ada peringkat
- To Control Nausea and Vomiting: Drug StudyDokumen2 halamanTo Control Nausea and Vomiting: Drug StudyPeace Andong PerochoBelum ada peringkat
- Chancroid TocDokumen12 halamanChancroid TocPeace Andong PerochoBelum ada peringkat
- Herpes ZosterDokumen3 halamanHerpes ZosterPeace Andong PerochoBelum ada peringkat
- DrugsDokumen2 halamanDrugsPeace Andong PerochoBelum ada peringkat
- Article Reaction Sa C.A. 2Dokumen8 halamanArticle Reaction Sa C.A. 2Peace Andong PerochoBelum ada peringkat
- LK BMHS 30 September 2021Dokumen71 halamanLK BMHS 30 September 2021samudraBelum ada peringkat
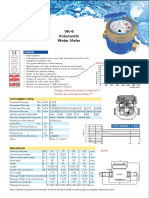
- Baylan: VK-6 Volumetric Water MeterDokumen1 halamanBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaBelum ada peringkat
- Portfolio Corporate Communication AuditDokumen8 halamanPortfolio Corporate Communication Auditapi-580088958Belum ada peringkat
- BSC in EEE Full Syllabus (Credit+sylabus)Dokumen50 halamanBSC in EEE Full Syllabus (Credit+sylabus)Sydur RahmanBelum ada peringkat
- SM 2021 MBA Assignment Forecasting InstructionsDokumen3 halamanSM 2021 MBA Assignment Forecasting InstructionsAmit Anand KumarBelum ada peringkat
- Questions For ReviewDokumen2 halamanQuestions For ReviewJoemar JavierBelum ada peringkat
- ITC Report and Accounts 2016Dokumen276 halamanITC Report and Accounts 2016Rohan SatijaBelum ada peringkat
- Analysis of Financial Ratios of Manufacturing CompaniesDokumen61 halamanAnalysis of Financial Ratios of Manufacturing CompaniesNine ZetBelum ada peringkat
- CP Exit Srategy Plan TemplateDokumen4 halamanCP Exit Srategy Plan TemplateKristia Stephanie BejeranoBelum ada peringkat
- AXIS Camera Station Installation and Migration Guide: User ManualDokumen7 halamanAXIS Camera Station Installation and Migration Guide: User ManualCORAL ALONSOBelum ada peringkat
- Lab Equipment Catalog Research Concept LabDokumen40 halamanLab Equipment Catalog Research Concept LabSeetanshu AwasthiBelum ada peringkat
- Ts 391 IltDokumen5 halamanTs 391 IltFunnypoumBelum ada peringkat
- SQL DBA Mod 1 IntroDokumen27 halamanSQL DBA Mod 1 IntroDivyaBelum ada peringkat
- Power Efficiency Diagnostics ReportDokumen16 halamanPower Efficiency Diagnostics Reportranscrib300Belum ada peringkat
- Ganbare Douki Chan MALDokumen5 halamanGanbare Douki Chan MALShivam AgnihotriBelum ada peringkat
- GFRDDokumen9 halamanGFRDLalit NagarBelum ada peringkat
- EPA - Regulatory Impact AnalysisDokumen822 halamanEPA - Regulatory Impact AnalysisSugarcaneBlogBelum ada peringkat
- Appendix 9A: Standard Specifications For Electrical DesignDokumen5 halamanAppendix 9A: Standard Specifications For Electrical Designzaheer ahamedBelum ada peringkat
- Naoh Storage Tank Design Description:: Calculations For Tank VolumeDokumen6 halamanNaoh Storage Tank Design Description:: Calculations For Tank VolumeMaria Eloisa Angelie ArellanoBelum ada peringkat
- Jurisdiction of The Supreme CourtDokumen1 halamanJurisdiction of The Supreme CourtAnshul Yadav100% (1)
- 231025+ +JBS+3Q23+Earnings+Preview VFDokumen3 halaman231025+ +JBS+3Q23+Earnings+Preview VFgicokobayashiBelum ada peringkat
- Timesheet 2021Dokumen1 halamanTimesheet 20212ys2njx57vBelum ada peringkat