Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- INFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Dokumen21 halamanINFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Si PuputBelum ada peringkat
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDokumen14 halamanRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputBelum ada peringkat
- Eye Health in The Commonwealth - Progress Report 2018 To 2020Dokumen30 halamanEye Health in The Commonwealth - Progress Report 2018 To 2020Si PuputBelum ada peringkat
- Current Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathyDokumen11 halamanCurrent Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathySi PuputBelum ada peringkat
- Towards Universal Eye Health Western PacificDokumen28 halamanTowards Universal Eye Health Western PacificSi PuputBelum ada peringkat
- Normal Postnatal Ocular DevelopmentDokumen23 halamanNormal Postnatal Ocular DevelopmentSi PuputBelum ada peringkat
- Duty Report 18 Januari 2020Dokumen13 halamanDuty Report 18 Januari 2020Si PuputBelum ada peringkat
- Rapid Sequence InductionDokumen2 halamanRapid Sequence InductionSi PuputBelum ada peringkat
- New Doc 2018-05-04Dokumen2 halamanNew Doc 2018-05-04Si PuputBelum ada peringkat
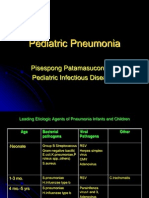
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDokumen39 halamanPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- US Army First Aid For Soldiers FM 21-11Dokumen243 halamanUS Army First Aid For Soldiers FM 21-11Total Prepper100% (2)
- 224 Closed Manipulation Casting of Distal Radius Fractures Fernandez DL 2005 Hand Clin p307-316 PDFDokumen10 halaman224 Closed Manipulation Casting of Distal Radius Fractures Fernandez DL 2005 Hand Clin p307-316 PDFanindyadputriBelum ada peringkat
- HAAD 100 Top Orthopaedics MCQ and AnswersDokumen18 halamanHAAD 100 Top Orthopaedics MCQ and AnswersAsif Newaz100% (3)
- Case Abstract Tibial FractureDokumen20 halamanCase Abstract Tibial FractureKceey CruzBelum ada peringkat
- CGHS Rate ListDokumen29 halamanCGHS Rate ListkkichaBelum ada peringkat
- Objective Questions For NursingDokumen53 halamanObjective Questions For NursingBIBI MOHANAN0% (1)
- Question OrthoDokumen4 halamanQuestion OrthoMohammed AbuzayedBelum ada peringkat
- Biology M10 Musculo-Skeletal SystemDokumen24 halamanBiology M10 Musculo-Skeletal SystemDiana Dealino-Sabandal100% (1)
- Musculoskeletal SystemDokumen22 halamanMusculoskeletal SystemKeyna DizonBelum ada peringkat
- Hip FractureDokumen4 halamanHip FractureJoel Vertt C. Balboa100% (1)
- Chapter 4 Surgery Musculoskeletal System CPT Codes 20000 - 29999Dokumen20 halamanChapter 4 Surgery Musculoskeletal System CPT Codes 20000 - 29999Rashiden MadjalesBelum ada peringkat
- POWEV2434234Dokumen461 halamanPOWEV2434234John M. HemsworthBelum ada peringkat
- Bryant's TractionDokumen2 halamanBryant's TractionGabbii CincoBelum ada peringkat
- 024344Dokumen6 halaman024344Aravind DesaiBelum ada peringkat
- Oet Reading 1 (A&b)Dokumen66 halamanOet Reading 1 (A&b)Richard James San JoseBelum ada peringkat
- Katalog Multiple Casualty Simulation KitDokumen1 halamanKatalog Multiple Casualty Simulation Kitwahyu sulistya affarahBelum ada peringkat
- First AidDokumen25 halamanFirst AidGaurav VermaBelum ada peringkat
- Basic of Manual TherapyDokumen30 halamanBasic of Manual Therapycamy bhagatBelum ada peringkat
- 3 Safety Device and Comfort MeasuresDokumen55 halaman3 Safety Device and Comfort MeasuresKaleb Ashiko100% (1)
- Orthopedic Radiographic in Exoctic Animal PracticeDokumen22 halamanOrthopedic Radiographic in Exoctic Animal PracticeHidaBelum ada peringkat
- n3021 Care Plan Week 2Dokumen7 halamann3021 Care Plan Week 2api-535585535Belum ada peringkat
- Fracture ManagementDokumen21 halamanFracture ManagementPatrickk WandererBelum ada peringkat
- TST D Scope Telescopic Nail EngDokumen28 halamanTST D Scope Telescopic Nail EngnorelBelum ada peringkat
- Sports Injuries: How Are Classified and Managed?Dokumen14 halamanSports Injuries: How Are Classified and Managed?Rachmat BayuBelum ada peringkat
- Helping Your Elbow To Recover After A Radial Head Fracture: Physiotherapy DepartmentDokumen8 halamanHelping Your Elbow To Recover After A Radial Head Fracture: Physiotherapy DepartmentJeongwoo PARKBelum ada peringkat
- Jdhodt 01 00025Dokumen6 halamanJdhodt 01 00025dithaBelum ada peringkat
- Bibliography of Orthopaedic Problems in Developing CountriesDokumen116 halamanBibliography of Orthopaedic Problems in Developing CountriesCristina IlieBelum ada peringkat
- AO Manual of Fracture Management - Internal Fixators, Thieme 2006-TLS (Michael Wagner)Dokumen889 halamanAO Manual of Fracture Management - Internal Fixators, Thieme 2006-TLS (Michael Wagner)Олексій ЮрченкоBelum ada peringkat
- PDF Khatri OdontoidFracturesDokumen65 halamanPDF Khatri OdontoidFracturesAlecsa Ana MariaBelum ada peringkat
- Rhombic 3D Condylar Fracture PlateDokumen8 halamanRhombic 3D Condylar Fracture PlateahujasurajBelum ada peringkat