Anda mungkin juga menyukai
- (HGT X 18.18) 140 Units 20Dokumen3 halaman(HGT X 18.18) 140 Units 20Jorelyn FriasBelum ada peringkat
- PSMID COVID TX Guidelines V.3.31.20a PDFDokumen62 halamanPSMID COVID TX Guidelines V.3.31.20a PDFRenz Marion AlemaniaBelum ada peringkat
- IM 3A - Pulmonology - Pneumonia PDFDokumen7 halamanIM 3A - Pulmonology - Pneumonia PDFJorelyn FriasBelum ada peringkat
- Im 3b-Pulmo Ratio FinalsDokumen382 halamanIm 3b-Pulmo Ratio FinalsJorelyn FriasBelum ada peringkat
- (Gyne) 3.4 Benign Gynecologic Lesions (LReyes) - Section3EDokumen22 halaman(Gyne) 3.4 Benign Gynecologic Lesions (LReyes) - Section3EJorelyn FriasBelum ada peringkat
- IM 3A - Pulmonology - Pneumonia PDFDokumen7 halamanIM 3A - Pulmonology - Pneumonia PDFJorelyn FriasBelum ada peringkat
- IM PULMO - PneumoniaDokumen9 halamanIM PULMO - PneumoniaJorelyn FriasBelum ada peringkat
- Hypothyroidism Signs and SymptomsDokumen11 halamanHypothyroidism Signs and SymptomsJorelyn Frias100% (1)
- Monitoring in AnesthesiaDokumen4 halamanMonitoring in AnesthesiaJorelyn FriasBelum ada peringkat
- (IM3b) Cardio Ratio FinalsDokumen354 halaman(IM3b) Cardio Ratio FinalsJorelyn FriasBelum ada peringkat
- Prelims 2015Dokumen18 halamanPrelims 2015Jorelyn FriasBelum ada peringkat
- CSF and CNS InfectionsDokumen9 halamanCSF and CNS InfectionsJorelyn Frias100% (1)
- Blood Physiology Part 2 Dr. OlivarDokumen5 halamanBlood Physiology Part 2 Dr. OlivarJorelyn FriasBelum ada peringkat
- 1.1 Renal Physio Pt. 1&2 - MarianoDokumen9 halaman1.1 Renal Physio Pt. 1&2 - MarianoJorelyn FriasBelum ada peringkat
- Seizure and EpilepsyDokumen7 halamanSeizure and EpilepsyJorelyn FriasBelum ada peringkat
- Pattern Before Present Interpretation AnalysisDokumen8 halamanPattern Before Present Interpretation AnalysisJorelyn FriasBelum ada peringkat
- Cardiodynamics - Dra-1. ValerioDokumen7 halamanCardiodynamics - Dra-1. ValerioJorelyn FriasBelum ada peringkat
- (PHYSIO B) 1.2 Renal Physio Pt. 3Dokumen8 halaman(PHYSIO B) 1.2 Renal Physio Pt. 3miguel cuevasBelum ada peringkat
- CA Lab ValuesDokumen8 halamanCA Lab ValuesJorelyn FriasBelum ada peringkat
- Respiratory PhysiologyDokumen137 halamanRespiratory PhysiologysramvigneshBelum ada peringkat
- Blood Physiology Part 1 Dr. OlivarDokumen10 halamanBlood Physiology Part 1 Dr. OlivarJorelyn FriasBelum ada peringkat
- (Gyne) 3.5 Neoplastic Diseases of The Ovary (LDReyes) - JTIIIDokumen7 halaman(Gyne) 3.5 Neoplastic Diseases of The Ovary (LDReyes) - JTIIIJorelyn FriasBelum ada peringkat
- Back Shoulder MusclesDokumen1 halamanBack Shoulder MusclesJorelyn FriasBelum ada peringkat
- Invasive Procedures HandoutsDokumen16 halamanInvasive Procedures HandoutsJorelyn FriasBelum ada peringkat
- Cardiologist Job DescriptionDokumen1 halamanCardiologist Job DescriptionJorelyn FriasBelum ada peringkat
- Rope Man ShipDokumen5 halamanRope Man ShipJorelyn FriasBelum ada peringkat
- Leadership Qualities and StylesDokumen10 halamanLeadership Qualities and StylesJorelyn FriasBelum ada peringkat
- Assessment A Critically Ill PatientDokumen23 halamanAssessment A Critically Ill PatientJorelyn Frias100% (1)
- Ch9-Stoichiometry 2Dokumen87 halamanCh9-Stoichiometry 2Jorelyn FriasBelum ada peringkat
- CA Lab ValuesDokumen8 halamanCA Lab ValuesJorelyn FriasBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hanoi 2023 Peoples Picks AwardsDokumen113 halamanHanoi 2023 Peoples Picks AwardsNguyen Anh VuBelum ada peringkat
- Assignment 1 Systems Analysis - EME5601Dokumen7 halamanAssignment 1 Systems Analysis - EME5601Travis GrantBelum ada peringkat
- IRELAND - Rivers, Lakes and Mountains: Look at The Maps and Answer These QuestionsDokumen2 halamanIRELAND - Rivers, Lakes and Mountains: Look at The Maps and Answer These QuestionsHannaBelum ada peringkat
- Mibk - TDS PDFDokumen3 halamanMibk - TDS PDFMardianus U. RihiBelum ada peringkat
- Casa Cook ArvindDokumen65 halamanCasa Cook ArvindLEAN MauritiusBelum ada peringkat
- Week 2 - Risk AssessmentDokumen35 halamanWeek 2 - Risk AssessmentTahir BashirBelum ada peringkat
- Astm F477-08Dokumen4 halamanAstm F477-08ALARCONISTABelum ada peringkat
- Explore the Precambrian EraDokumen3 halamanExplore the Precambrian EraArjay CarolinoBelum ada peringkat
- CHM4943 Wastewater TreatmentDokumen7 halamanCHM4943 Wastewater TreatmentUsman GhaniBelum ada peringkat
- 2G - 4G Network Module - Data Sheet - EnglishDokumen8 halaman2G - 4G Network Module - Data Sheet - EnglishbbwroBelum ada peringkat
- Land Rover Range Rover Owners Manual 2007Dokumen358 halamanLand Rover Range Rover Owners Manual 2007PetreCaracaleanu0% (1)
- RenderingDokumen6 halamanRenderingJuno PajelBelum ada peringkat
- Chapter 6 Exercises (Bonds & Interest)Dokumen2 halamanChapter 6 Exercises (Bonds & Interest)Shaheera SuhaimiBelum ada peringkat
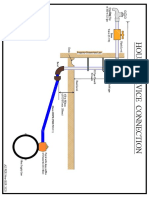
- House Service Connection NEW BSR 2020-1Dokumen1 halamanHouse Service Connection NEW BSR 2020-1Deshraj BairwaBelum ada peringkat
- A Community School: Research Aspect 2 ReportDokumen13 halamanA Community School: Research Aspect 2 ReportMarsha MianBelum ada peringkat
- ImmortalDokumen4 halamanImmortalMaNithyaVishalanandaBelum ada peringkat
- FH400 73158464 Pca-6.140Dokumen431 halamanFH400 73158464 Pca-6.140IgorGorduz100% (1)
- Comp7 - Answer Key - Dec. Exam - 1st SetDokumen2 halamanComp7 - Answer Key - Dec. Exam - 1st SetHazel Joy LusellaBelum ada peringkat
- Ring OnlyDokumen2 halamanRing Onlyapi-3834777Belum ada peringkat
- Transmission Lines Explained for Efficiency and Loss ReductionDokumen25 halamanTransmission Lines Explained for Efficiency and Loss Reductionjagdish choudharyBelum ada peringkat
- Curriculum Vitae of Masilo ModibaDokumen11 halamanCurriculum Vitae of Masilo Modibalevy2011Belum ada peringkat
- W2AEW Videos (Apr 29, 2017) Topics Listed NumericallyDokumen12 halamanW2AEW Videos (Apr 29, 2017) Topics Listed Numericallyamol1agarwalBelum ada peringkat
- Minicap FTC260, FTC262: Technical InformationDokumen20 halamanMinicap FTC260, FTC262: Technical InformationAmanda PorterBelum ada peringkat
- Complete The Table With The Missing WordsDokumen2 halamanComplete The Table With The Missing WordssoniaBelum ada peringkat
- Cap Tikus As Symbol of Social Closeness in The Life of The Minahasa PeopleDokumen3 halamanCap Tikus As Symbol of Social Closeness in The Life of The Minahasa PeopleEdwinBelum ada peringkat
- CH 2 Atoms, Ions, and MoleculesDokumen64 halamanCH 2 Atoms, Ions, and MoleculesBritney SimmsBelum ada peringkat
- EV1116 Manual 146251999-4DDokumen32 halamanEV1116 Manual 146251999-4Danitha ferryBelum ada peringkat
- 2003 VW Jetta Wiring DiagramsDokumen123 halaman2003 VW Jetta Wiring DiagramsmikeBelum ada peringkat
- SmogDokumen5 halamanSmogAlain MoratallaBelum ada peringkat
- 2G Call FlowDokumen71 halaman2G Call Flowm191084Belum ada peringkat