Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- GST 101Dokumen247 halamanGST 101Emmanuel Adewale Sanda100% (2)
- Buss Barnes 1986 PDFDokumen12 halamanBuss Barnes 1986 PDFAna MirelaBelum ada peringkat
- Cosmetics in Shakespearean and Renaissance DramaDokumen233 halamanCosmetics in Shakespearean and Renaissance Dramatlbaocvrvd100% (1)
- Vertigo Perifer: Case Report SessionDokumen1 halamanVertigo Perifer: Case Report SessionEko RizkiBelum ada peringkat
- Demam Berdarah Dengue: Case Report SessionDokumen1 halamanDemam Berdarah Dengue: Case Report SessionEko RizkiBelum ada peringkat
- Case Report Session (Group II) : Preseptor: Prof - Dr. H. Basjiruddin Ahmad, SP.S (K)Dokumen19 halamanCase Report Session (Group II) : Preseptor: Prof - Dr. H. Basjiruddin Ahmad, SP.S (K)Eko RizkiBelum ada peringkat
- What Is Diabetes?: Here Are Some Interesting Facts!Dokumen2 halamanWhat Is Diabetes?: Here Are Some Interesting Facts!Eko RizkiBelum ada peringkat
- No HPDokumen4 halamanNo HPEko RizkiBelum ada peringkat
- Fisiologi Penuaan Normal: Rahmatina B. Herman Fakultas Kedokteran Universitas AndalasDokumen24 halamanFisiologi Penuaan Normal: Rahmatina B. Herman Fakultas Kedokteran Universitas AndalasEko RizkiBelum ada peringkat
- Fka FKB Fke FKF Fki FKJ FKM FKNDokumen1 halamanFka FKB Fke FKF Fki FKJ FKM FKNEko RizkiBelum ada peringkat
- Body Esteem ScaleDokumen2 halamanBody Esteem Scaleamansharma0007Belum ada peringkat
- June 2018 QP - Biology 1 (H) Edexcel Science GCSEDokumen24 halamanJune 2018 QP - Biology 1 (H) Edexcel Science GCSESHOABBelum ada peringkat
- Theories of Mate SelectionDokumen4 halamanTheories of Mate SelectionbabeBelum ada peringkat
- Nutritional Status ReportDokumen1 halamanNutritional Status ReportEL JEAH MOSQUEDABelum ada peringkat
- 2nd LessonDokumen21 halaman2nd LessonArjay Dela CruzBelum ada peringkat
- Body Mass Index Calculator (BMI) A J Hedges: WWW - Hedgeshypnosis.co - UkDokumen2 halamanBody Mass Index Calculator (BMI) A J Hedges: WWW - Hedgeshypnosis.co - UkRohizamBelum ada peringkat
- Salter Scales 9117Dokumen10 halamanSalter Scales 9117695gowerBelum ada peringkat
- Inbody 12 - 07 - 21Dokumen1 halamanInbody 12 - 07 - 21Mahdi GuenifiBelum ada peringkat
- Talley and O'Connor's Clinical Examination 8th Edition PDFDriveDokumen8 halamanTalley and O'Connor's Clinical Examination 8th Edition PDFDriveSyaza SyedBelum ada peringkat
- Use WEIGHT-FOR-LENGTH or WEIGHT-FOR-HEIGHT To Correctly Determine Overweight and ObesityDokumen3 halamanUse WEIGHT-FOR-LENGTH or WEIGHT-FOR-HEIGHT To Correctly Determine Overweight and ObesityExzur ChavezBelum ada peringkat
- WorkZine 64Dokumen18 halamanWorkZine 64TheRealWorkZineBelum ada peringkat
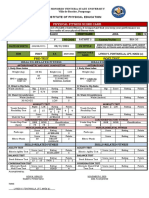
- Pre-Test Post Test: Physical Fitness Score CardDokumen2 halamanPre-Test Post Test: Physical Fitness Score CardRed CactusBelum ada peringkat
- RULES Athletes 2015Dokumen15 halamanRULES Athletes 2015Wow FitBelum ada peringkat
- Lifestyle and Weight Management-EditedDokumen26 halamanLifestyle and Weight Management-EditedkitcathBelum ada peringkat
- Bio Lab 3Dokumen4 halamanBio Lab 3Nkosi Jupiter100% (1)
- Human RelationshipsDokumen16 halamanHuman RelationshipsAsmita MundheBelum ada peringkat
- Ideal Weight ChartDokumen4 halamanIdeal Weight ChartMarvin Osmar Estrada JuarezBelum ada peringkat
- Nutritional Status Report of Dapdap Elementary High School: TotalDokumen2 halamanNutritional Status Report of Dapdap Elementary High School: TotalAnalyn PenarandaBelum ada peringkat
- The Americanization of Beauty Standards: Beauty Perceptions Between The Socioeconomic Classes in Costa RicaDokumen8 halamanThe Americanization of Beauty Standards: Beauty Perceptions Between The Socioeconomic Classes in Costa Ricaaleksfonse100% (1)
- Assignment/ Tugasan - Health and Wellness 2Dokumen14 halamanAssignment/ Tugasan - Health and Wellness 2Metran Electrical & ITBelum ada peringkat
- 15 Body Types & WeightDokumen29 halaman15 Body Types & Weightapi-286702267Belum ada peringkat
- Body Types MCQDokumen9 halamanBody Types MCQDoha DharewaBelum ada peringkat
- How Is The Poem Phenomenal Woman' A Reflection of The Poet's Personal Life?Dokumen5 halamanHow Is The Poem Phenomenal Woman' A Reflection of The Poet's Personal Life?SourodipKundu100% (1)
- Grade 7 NS Baseline 202022 2023Dokumen2 halamanGrade 7 NS Baseline 202022 2023DIOSA N.CAPISTRANOBelum ada peringkat
- Tablas OMSDokumen46 halamanTablas OMSalan tolentinoBelum ada peringkat
- Biggest LoserDokumen173 halamanBiggest LoserLynseyBelum ada peringkat
- Kurva Pertumbuhan WHODokumen12 halamanKurva Pertumbuhan WHOAzmi LarasatiBelum ada peringkat