Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Rehabilitation After Multiple-Ligament ReconstructionDokumen5 halamanRehabilitation After Multiple-Ligament ReconstructionvarahamihirBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Reporting The Results of Clinical ResearchDokumen16 halamanReporting The Results of Clinical ResearchvarahamihirBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Pathophysiology of Spastic Paresis IDokumen17 halamanPathophysiology of Spastic Paresis Ivarahamihir100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Measure School Learning Through Rasch AnalysisDokumen5 halamanMeasure School Learning Through Rasch AnalysisvarahamihirBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- NHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)Dokumen21 halamanNHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)varahamihirBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Application of Rasch Analysis in The Development and Application of Quality of Life InstrumentsDokumen5 halamanApplication of Rasch Analysis in The Development and Application of Quality of Life InstrumentsvarahamihirBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Physiological and Physical Determinants - Juvenile DermatomyositisDokumen16 halamanPhysiological and Physical Determinants - Juvenile DermatomyositisvarahamihirBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Gait in Children With Cerebral PalsyDokumen5 halamanGait in Children With Cerebral PalsyvarahamihirBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Zoology Notes on Physiology, Anatomy and GeneticsDokumen11 halamanZoology Notes on Physiology, Anatomy and GeneticskrishnaBelum ada peringkat
- (S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Dokumen28 halaman(S-W5-Sun-Gen.S) (By Dr. Emad) Gall Bladder 1Haider Nadhem AL-rubaiBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- A. Menstrual Cycle Here Are Important Events During The Menstrual CycleDokumen2 halamanA. Menstrual Cycle Here Are Important Events During The Menstrual CycleRosiro33% (3)
- Ap Psychology Unit 7 Overview Revised 2015Dokumen5 halamanAp Psychology Unit 7 Overview Revised 2015api-262090199Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Class HolothuroideaDokumen2 halamanClass HolothuroideaSecretsoushiBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Abdominal NodesDokumen8 halamanAbdominal NodesatihsaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Surface Anatomy of The HeartDokumen5 halamanSurface Anatomy of The HeartEglBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- EmbolismDokumen11 halamanEmbolismSubhrajyoti RoyBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Digestion and Absorption: Fact/Definition Type QuestionsDokumen9 halamanDigestion and Absorption: Fact/Definition Type QuestionsNayan BhardwazBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The "Ballista Spring" System For Impacted Teeth: Genevu. SwitzerlandDokumen9 halamanThe "Ballista Spring" System For Impacted Teeth: Genevu. Switzerlandapi-26468957100% (1)
- Student Thesis AssessmentDokumen3 halamanStudent Thesis AssessmentAnggi Anggraeni Ratu GumelarBelum ada peringkat
- The Digestive System Powerpoint 1227698045024899 8Dokumen44 halamanThe Digestive System Powerpoint 1227698045024899 8SunnyReduBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Mechanisms of Coagulation and Fibrinolysis (Autosaved)Dokumen60 halamanMechanisms of Coagulation and Fibrinolysis (Autosaved)Tom Anthony TonguiaBelum ada peringkat
- Pes 2023Dokumen1 halamanPes 2023dr_yasserBelum ada peringkat
- Manage Endocrine DisordersDokumen2 halamanManage Endocrine DisordersJan Cyrel ColomaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
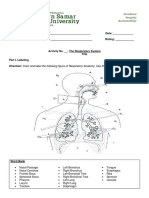
- The Respiratory System ActivityDokumen4 halamanThe Respiratory System ActivityVina DiscarBelum ada peringkat
- Chronic Hyperplastic PulpitisDokumen30 halamanChronic Hyperplastic PulpitisGlory Pohan67% (3)
- Residency 1000 QuestionDokumen599 halamanResidency 1000 QuestionTan 57Belum ada peringkat
- Urinary SystemDokumen9 halamanUrinary SystemCailah Sofia SelausoBelum ada peringkat
- Curs5 Hematologie AnvDokumen59 halamanCurs5 Hematologie AnvRaluca PăunaBelum ada peringkat
- Secretory Functions of GITDokumen24 halamanSecretory Functions of GITDr.Nusrat TariqBelum ada peringkat
- Discussion Questions - Chapter 2Dokumen6 halamanDiscussion Questions - Chapter 2nlenz94Belum ada peringkat
- Endocrine System Chapter SummaryDokumen6 halamanEndocrine System Chapter SummaryShiny ChenBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- ProcreationDokumen55 halamanProcreationRoshin TejeroBelum ada peringkat
- DCM Medical Secretary - Glossary - Medical Terms PDFDokumen71 halamanDCM Medical Secretary - Glossary - Medical Terms PDFEoin O'Byrne100% (1)
- Brain Parts and Functions ExplainedDokumen4 halamanBrain Parts and Functions ExplainedRose TuludBelum ada peringkat
- Apraxia PDFDokumen13 halamanApraxia PDFAndré CantanhedeBelum ada peringkat
- FCD (SA) OMP Regulations 24-3-2014Dokumen9 halamanFCD (SA) OMP Regulations 24-3-2014matentenBelum ada peringkat
- BY Janani.N Omfs PGDokumen15 halamanBY Janani.N Omfs PGjanani narayananBelum ada peringkat
- (K4) Male Reproductive SystemDokumen73 halaman(K4) Male Reproductive SystemJane Andrea Christiano DjianzonieBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)