Anda mungkin juga menyukai
- The Successful Treatment of DisinhibitioDokumen4 halamanThe Successful Treatment of DisinhibitioVicky NotesBelum ada peringkat
- Schizoaffective Disorder: Continuing Education ActivityDokumen10 halamanSchizoaffective Disorder: Continuing Education ActivitymusdalifahBelum ada peringkat
- Literature Review SchizophreniaDokumen5 halamanLiterature Review Schizophreniaafmzuiffugjdff100% (1)
- Esquizofrenia InglesDokumen5 halamanEsquizofrenia Ingleseve-16Belum ada peringkat
- Dementia Due To NeurosyphilisDokumen3 halamanDementia Due To NeurosyphilisIOSRjournalBelum ada peringkat
- Understanding Schizophrenia Through a Case StudyDokumen22 halamanUnderstanding Schizophrenia Through a Case StudyAinal MardhiyyahBelum ada peringkat
- LIDZ THEODORE - A Psicosocial Orientation To Schizophrenic DisordersDokumen9 halamanLIDZ THEODORE - A Psicosocial Orientation To Schizophrenic DisordersRodrigo G.Belum ada peringkat
- SchizophreniaDokumen21 halamanSchizophreniapriya hemBelum ada peringkat
- Overview and Treatment Option: SkizofreniaDokumen8 halamanOverview and Treatment Option: SkizofreniaEvi LoBelum ada peringkat
- Major Self-Mutilation in The First Episode of PsychosisDokumen10 halamanMajor Self-Mutilation in The First Episode of PsychosisJulián EspinalBelum ada peringkat
- Van Os J, Kapur S. Schizophrenia - Lancet 2009 374 635-45 PDFDokumen11 halamanVan Os J, Kapur S. Schizophrenia - Lancet 2009 374 635-45 PDFVictorVeroneseBelum ada peringkat
- Neuropsychiatric Sequelae of Nipah Virus Encephalitis: MethodsDokumen5 halamanNeuropsychiatric Sequelae of Nipah Virus Encephalitis: MethodsTryas YulithaBelum ada peringkat
- Vol 54 No 2 Patel Selby YekkiralaDokumen5 halamanVol 54 No 2 Patel Selby YekkiralaDrashua AshuaBelum ada peringkat
- Refining CBT for Persistent Positive Symptoms in PsychosisDokumen8 halamanRefining CBT for Persistent Positive Symptoms in PsychosisvinodksahuBelum ada peringkat
- Schizophrenia etiology, symptoms, treatmentDokumen12 halamanSchizophrenia etiology, symptoms, treatmentmustafa566512345Belum ada peringkat
- Schizophrenia Patients' Cognition vs. Healthy IndividualsDokumen6 halamanSchizophrenia Patients' Cognition vs. Healthy IndividualsAsti DwiningsihBelum ada peringkat
- 5ch Izoph Ren Ia: Key ConceptsDokumen24 halaman5ch Izoph Ren Ia: Key ConceptsNAURA ARNEITA AN-NAJLABelum ada peringkat
- Psychotic Symptoms As A Continuum Between Normality and PathologyDokumen12 halamanPsychotic Symptoms As A Continuum Between Normality and PathologyOana OrosBelum ada peringkat
- Schizophr Bull 2011 Simonsen 73 83Dokumen11 halamanSchizophr Bull 2011 Simonsen 73 83Tara WandhitaBelum ada peringkat
- CJP May 06 Chaudhari OR7Dokumen8 halamanCJP May 06 Chaudhari OR7haddig8Belum ada peringkat
- Genetics, Cognition, and Neurobiology of Schizotypal Personality: A Review of The Overlap With SchizophreniaDokumen16 halamanGenetics, Cognition, and Neurobiology of Schizotypal Personality: A Review of The Overlap With SchizophreniaDewi NofiantiBelum ada peringkat
- Schizophrenia: Clinical ReviewDokumen5 halamanSchizophrenia: Clinical ReviewPuji Arifianti RamadhanyBelum ada peringkat
- Psychiatric Disorders Associated With EpilepsyDokumen18 halamanPsychiatric Disorders Associated With EpilepsyAllan DiasBelum ada peringkat
- SCHIZOPHRENIFORMDokumen5 halamanSCHIZOPHRENIFORMThrift AdvisoryBelum ada peringkat
- A Talking Cure For PsychosisDokumen6 halamanA Talking Cure For PsychosisKarla ValderramaBelum ada peringkat
- New-Onset: Hallucinations Patients Infected WithDokumen6 halamanNew-Onset: Hallucinations Patients Infected Withtugba1234Belum ada peringkat
- Swinkels PscychopathologieDokumen16 halamanSwinkels PscychopathologiesezalwickBelum ada peringkat
- Bipolaridade e Esclerose MúltiplaDokumen4 halamanBipolaridade e Esclerose MúltiplaLucasFelipeRibeiroBelum ada peringkat
- Psychiatric effects of thyroid hormone disturbanceDokumen9 halamanPsychiatric effects of thyroid hormone disturbanceJosetta WhitneyBelum ada peringkat
- Steroid-Induced PsychosisDokumen2 halamanSteroid-Induced Psychosisanisha batraBelum ada peringkat
- Schizophrenia JAUHAR Publishedonline28January2022 GREEN AAMDokumen44 halamanSchizophrenia JAUHAR Publishedonline28January2022 GREEN AAMAlondra CastilloBelum ada peringkat
- Psychobiology Schizophrenia Research Paper FINAL (At)Dokumen8 halamanPsychobiology Schizophrenia Research Paper FINAL (At)gucci maneBelum ada peringkat
- Neurosyphilis: The Reemergence of An Historical DiseaseDokumen2 halamanNeurosyphilis: The Reemergence of An Historical DiseaseDrashua AshuaBelum ada peringkat
- Case Study LnaDokumen13 halamanCase Study LnaSarah Y AL-SalahatBelum ada peringkat
- Neurotransmitters and SuicideDokumen24 halamanNeurotransmitters and Suicide9rvvgf5vx8Belum ada peringkat
- Roberts Psychiatric 1992Dokumen3 halamanRoberts Psychiatric 1992Drashua AshuaBelum ada peringkat
- Kazkas Su Alcohol PDFDokumen5 halamanKazkas Su Alcohol PDFMartis JonasBelum ada peringkat
- Bipolar DisorderDokumen20 halamanBipolar Disorderabk52166Belum ada peringkat
- Ltz-Psychodiagnostics Intro-Evolution, Growth and DevelopmentDokumen88 halamanLtz-Psychodiagnostics Intro-Evolution, Growth and DevelopmentLucy RalteBelum ada peringkat
- Fernando - Waters2014Dokumen13 halamanFernando - Waters2014fernandogfcnsBelum ada peringkat
- Psychogenic DystoniaDokumen2 halamanPsychogenic DystoniaTomiuc AndreiBelum ada peringkat
- Neurosyphilis Presenting As Psychiatric Symptoms - An Unusual Case ReportDokumen3 halamanNeurosyphilis Presenting As Psychiatric Symptoms - An Unusual Case ReportKinga KlimczykBelum ada peringkat
- Related LiteratureDokumen16 halamanRelated LiteratureivahcamilleBelum ada peringkat
- Psychosurgery, Epilepsy Surgery, or Surgical Psychiatry: The Tangled Web of Epilepsy and Psychiatry As Revealed by Surgical OutcomesDokumen2 halamanPsychosurgery, Epilepsy Surgery, or Surgical Psychiatry: The Tangled Web of Epilepsy and Psychiatry As Revealed by Surgical Outcomesximena sanchezBelum ada peringkat
- Biomarcadores Neuroinmunes en Esquizofrenia. 2014Dokumen11 halamanBiomarcadores Neuroinmunes en Esquizofrenia. 2014Stephanie LandaBelum ada peringkat
- Pappolla Familial Hypercholesterolemia and Mild Cognitive ImpairmentDokumen13 halamanPappolla Familial Hypercholesterolemia and Mild Cognitive ImpairmentMike Pappolla MD, PhDBelum ada peringkat
- Schizophrenia: Overview and Treatment OptionsDokumen18 halamanSchizophrenia: Overview and Treatment OptionsMeindayaniBelum ada peringkat
- CH 4Dokumen11 halamanCH 4Usman khalidBelum ada peringkat
- Popovic Et Al-2014-Acta Psychiatrica ScandinavicaDokumen9 halamanPopovic Et Al-2014-Acta Psychiatrica ScandinavicaCarolina MuñozBelum ada peringkat
- Schizophrenia UndifferentiatedDokumen64 halamanSchizophrenia UndifferentiatedJen GarzoBelum ada peringkat
- Schizophrenia:Courseoverthe Lifetime: Philipd - Harvey MichaeldavidsonDokumen16 halamanSchizophrenia:Courseoverthe Lifetime: Philipd - Harvey MichaeldavidsonGeorgiana BlagociBelum ada peringkat
- Atypical antipsychotics for schizophrenia and substance abuseDokumen14 halamanAtypical antipsychotics for schizophrenia and substance abusecupin 69PKBelum ada peringkat
- 52 Tripathy EtalDokumen5 halaman52 Tripathy EtaleditorijmrhsBelum ada peringkat
- Course of OCDDokumen16 halamanCourse of OCDShwetank BansalBelum ada peringkat
- Psychosis and Seizure Disorder: Challenges in Diagnosis and TreatmentDokumen7 halamanPsychosis and Seizure Disorder: Challenges in Diagnosis and TreatmentgreenanubisBelum ada peringkat
- Jamapsychiatry 2019 3360Dokumen10 halamanJamapsychiatry 2019 3360Furqan BansirBelum ada peringkat
- Neurobiology of SchizophreniaDokumen11 halamanNeurobiology of SchizophreniaJerry JacobBelum ada peringkat
- Handbook of Medical Neuropsychology: Applications of Cognitive NeuroscienceDari EverandHandbook of Medical Neuropsychology: Applications of Cognitive NeuroscienceBelum ada peringkat
- Psychoanalysis (Barnes & Noble Digital Library): Its Theories and Practical Application, Third EditionDari EverandPsychoanalysis (Barnes & Noble Digital Library): Its Theories and Practical Application, Third EditionBelum ada peringkat
- Keys CardiologyDokumen1 halamanKeys CardiologyDrashua AshuaBelum ada peringkat
- DM CardiologyDokumen39 halamanDM CardiologyDrashua AshuaBelum ada peringkat
- Bence Jones Protein-UrineDokumen16 halamanBence Jones Protein-UrineDrashua Ashua100% (2)
- Post Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Dokumen1 halamanPost Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaBelum ada peringkat
- ABO in The Context ofDokumen21 halamanABO in The Context ofDrashua AshuaBelum ada peringkat
- Compliance rate study of bio-medical waste segregationDokumen50 halamanCompliance rate study of bio-medical waste segregationAman Dheer Kapoor100% (2)
- Bihar PG15 ProspectusDokumen37 halamanBihar PG15 ProspectusDrashua AshuaBelum ada peringkat
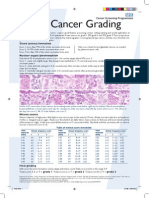
- Breast Cancer Grading PDFDokumen1 halamanBreast Cancer Grading PDFDrashua AshuaBelum ada peringkat
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Dokumen2 halamanPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaBelum ada peringkat
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Dokumen2 halamanPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaBelum ada peringkat
- Muscle Origins and InsertionsDokumen9 halamanMuscle Origins and Insertionsnoisytaost92% (12)
- HematologyDokumen58 halamanHematologyAchmad DainuriBelum ada peringkat
- Telephone Directory EngDokumen8 halamanTelephone Directory EngDrashua AshuaBelum ada peringkat
- CBD FullDokumen5 halamanCBD FullDrashua AshuaBelum ada peringkat
- Bio Medical Rules PDFDokumen28 halamanBio Medical Rules PDFDrashua AshuaBelum ada peringkat
- Hilgendorf Bio 07Dokumen52 halamanHilgendorf Bio 07Drashua AshuaBelum ada peringkat
- Shigella BackgroundDokumen2 halamanShigella BackgroundDrashua AshuaBelum ada peringkat
- Application PDFDokumen2 halamanApplication PDFDrashua AshuaBelum ada peringkat
- SHIGELLOSISDokumen1 halamanSHIGELLOSISDrashua AshuaBelum ada peringkat
- P 133-1430Dokumen11 halamanP 133-1430Drashua AshuaBelum ada peringkat
- ID 20i2.1Dokumen12 halamanID 20i2.1Drashua AshuaBelum ada peringkat
- Ecp Shigella InfectionDokumen4 halamanEcp Shigella InfectionDrashua AshuaBelum ada peringkat
- P 133-1430Dokumen11 halamanP 133-1430Drashua AshuaBelum ada peringkat
- Shigella in Child-Care SettingsDokumen2 halamanShigella in Child-Care SettingsDrashua AshuaBelum ada peringkat
- ShigellaDokumen1 halamanShigellaDrashua AshuaBelum ada peringkat
- Shige LLDokumen7 halamanShige LLDrashua AshuaBelum ada peringkat
- 420 079 Guideline ShigellosisDokumen7 halaman420 079 Guideline ShigellosisDrashua AshuaBelum ada peringkat
- Shigellosis: Frequently Asked QuestionsDokumen2 halamanShigellosis: Frequently Asked QuestionsDrashua AshuaBelum ada peringkat
- ShigellaDokumen2 halamanShigellaDrashua AshuaBelum ada peringkat
- 0314Dokumen6 halaman0314Drashua AshuaBelum ada peringkat
- dlp4 Math7q3Dokumen3 halamandlp4 Math7q3Therence UbasBelum ada peringkat
- MT 1 Combined Top 200Dokumen3 halamanMT 1 Combined Top 200ShohanBelum ada peringkat
- Garner Fructis ShampooDokumen3 halamanGarner Fructis Shampooyogesh0794Belum ada peringkat
- Unit 5 The Teacher As ProfessionalDokumen23 halamanUnit 5 The Teacher As ProfessionalLeame Hoyumpa Mazo100% (5)
- Sample Detailed EvaluationDokumen5 halamanSample Detailed Evaluationits4krishna3776Belum ada peringkat
- English FinalDokumen321 halamanEnglish FinalManuel Campos GuimeraBelum ada peringkat
- Mexican Immigrants and The Future of The American Labour Market (Schlossplatz3-Issue 8)Dokumen1 halamanMexican Immigrants and The Future of The American Labour Market (Schlossplatz3-Issue 8)Carlos J. GuizarBelum ada peringkat
- Here Late?", She Asked Me.: TrangDokumen3 halamanHere Late?", She Asked Me.: TrangNguyễn Đình TrọngBelum ada peringkat
- Alluring 60 Dome MosqueDokumen6 halamanAlluring 60 Dome Mosqueself sayidBelum ada peringkat
- Comparing and contrasting inductive learning and concept attainment strategiesDokumen3 halamanComparing and contrasting inductive learning and concept attainment strategiesKeira DesameroBelum ada peringkat
- Dead Can Dance - How Fortunate The Man With None LyricsDokumen3 halamanDead Can Dance - How Fortunate The Man With None LyricstheourgikonBelum ada peringkat
- Adult Education and Training in Europe 2020 21Dokumen224 halamanAdult Education and Training in Europe 2020 21Măndița BaiasBelum ada peringkat
- Infinitive Clauses PDFDokumen3 halamanInfinitive Clauses PDFKatia LeliakhBelum ada peringkat
- AL E C Usda S W P: OOK AT THE Ngineering Hallenges OF THE Mall Atershed RogramDokumen6 halamanAL E C Usda S W P: OOK AT THE Ngineering Hallenges OF THE Mall Atershed RogramFranciscoBelum ada peringkat
- History: The Origin of Kho-KhotheDokumen17 halamanHistory: The Origin of Kho-KhotheIndrani BhattacharyaBelum ada peringkat
- Research 2020.21 Outline PDFDokumen12 halamanResearch 2020.21 Outline PDFCharles MaherBelum ada peringkat
- Corporate Office Design GuideDokumen23 halamanCorporate Office Design GuideAshfaque SalzBelum ada peringkat
- Piramal Annual ReportDokumen390 halamanPiramal Annual ReportTotmolBelum ada peringkat
- Effective Instruction OverviewDokumen5 halamanEffective Instruction Overviewgene mapaBelum ada peringkat
- FOREIGN DOLL CORP May 2023 TD StatementDokumen4 halamanFOREIGN DOLL CORP May 2023 TD Statementlesly malebrancheBelum ada peringkat
- Álvaro García Linera A Marxist Seduced BookDokumen47 halamanÁlvaro García Linera A Marxist Seduced BookTomás TorresBelum ada peringkat
- Financial Management Module - 3Dokumen2 halamanFinancial Management Module - 3Roel AsduloBelum ada peringkat
- 3 QDokumen2 halaman3 QJerahmeel CuevasBelum ada peringkat
- Alsa Alsatom MB, MC - Service ManualDokumen26 halamanAlsa Alsatom MB, MC - Service ManualJoão Francisco MontanhaniBelum ada peringkat
- Lab Report FormatDokumen2 halamanLab Report Formatapi-276658659Belum ada peringkat
- JDDokumen19 halamanJDJuan Carlo CastanedaBelum ada peringkat
- MEAB Enewsletter 14 IssueDokumen5 halamanMEAB Enewsletter 14 Issuekristine8018Belum ada peringkat
- iPhone Repair FormDokumen1 halamaniPhone Repair Formkabainc0% (1)
- Block 2 MVA 026Dokumen48 halamanBlock 2 MVA 026abhilash govind mishraBelum ada peringkat
- The Wavy Tunnel: Trade Management Jody SamuelsDokumen40 halamanThe Wavy Tunnel: Trade Management Jody SamuelsPeter Nguyen100% (1)