Anda mungkin juga menyukai
- Vitamin TherapyDokumen4 halamanVitamin TherapyNNRWCBelum ada peringkat
- 40 Years of Evidence of RecoveryDokumen10 halaman40 Years of Evidence of RecoveryNNRWCBelum ada peringkat
- A Utah Juvenile Court Case StudyDokumen18 halamanA Utah Juvenile Court Case StudyNNRWCBelum ada peringkat
- Dr. Alfonso Paredes, Descriptive OverviewDokumen16 halamanDr. Alfonso Paredes, Descriptive OverviewNNRWCBelum ada peringkat
- Narconon Science ReferencesDokumen14 halamanNarconon Science ReferencesNNRWCBelum ada peringkat
- Summary of Ongoing EvaluationsDokumen3 halamanSummary of Ongoing EvaluationsNNRWCBelum ada peringkat
- Ongoing Program EvaluationDokumen6 halamanOngoing Program EvaluationNNRWCBelum ada peringkat
- Literature Supporting Detox ProgramDokumen5 halamanLiterature Supporting Detox ProgramNNRWCBelum ada peringkat
- Curriculum For High School StudentsDokumen6 halamanCurriculum For High School StudentsNNRWCBelum ada peringkat
- Ending Drug CravingsDokumen4 halamanEnding Drug CravingsNNRWCBelum ada peringkat
- Fat Stored XenobioticsDokumen14 halamanFat Stored XenobioticsNNRWCBelum ada peringkat
- Case Histories Part 2Dokumen3 halamanCase Histories Part 2NNRWCBelum ada peringkat
- Managing Chronic Ilness in PatientsDokumen9 halamanManaging Chronic Ilness in PatientsNNRWCBelum ada peringkat
- Detoxification: Metals, Pesticides, ChemicalsDokumen3 halamanDetoxification: Metals, Pesticides, ChemicalsNNRWCBelum ada peringkat
- Case Histories: Part 1Dokumen2 halamanCase Histories: Part 1NNRWCBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Active Learning StrategiesDokumen5 halamanActive Learning StrategiesQushoy Al IhsaniyBelum ada peringkat
- Engaging ParentsDokumen12 halamanEngaging Parentsapi-530935463Belum ada peringkat
- Benefits and Challenges of Women in University EducationDokumen3 halamanBenefits and Challenges of Women in University EducationTheMustardCatBelum ada peringkat
- Example of A Personal Statement For An NQT Primary PoolDokumen3 halamanExample of A Personal Statement For An NQT Primary PoolKantha Roa75% (4)
- Argument Essay Final DraftDokumen5 halamanArgument Essay Final Draftapi-575360331Belum ada peringkat
- Byjus Akaksh MergerDokumen2 halamanByjus Akaksh MergerPoulami DwibediBelum ada peringkat
- Travel & Tourism AS:A Level (9395) - 2024:2026 SyllabusDokumen48 halamanTravel & Tourism AS:A Level (9395) - 2024:2026 Syllabusyak0% (1)
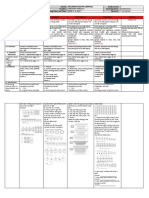
- 6 DLL - Math 2 - Q1 - W1Dokumen10 halaman6 DLL - Math 2 - Q1 - W1Eda Concepcion PalenBelum ada peringkat
- DO No. 76 S. 2010 Policy Guidelines UBDDokumen1 halamanDO No. 76 S. 2010 Policy Guidelines UBDBrayBelum ada peringkat
- DLL 2nd Quarter Wk2Dokumen6 halamanDLL 2nd Quarter Wk2KatherineNuescaBelum ada peringkat
- Silabus Speaking BasicDokumen2 halamanSilabus Speaking BasicAisil AmaniBelum ada peringkat
- Teaching GrammarDokumen45 halamanTeaching Grammardunkik100% (1)
- Final Project Lesson PlanDokumen2 halamanFinal Project Lesson Planapi-355214510Belum ada peringkat
- VRTC - LET Online Review ProgramDokumen14 halamanVRTC - LET Online Review ProgramMaria Garcia Pimentel Vanguardia IIBelum ada peringkat
- AHRM SyllabusDokumen2 halamanAHRM SyllabusKhalil GhazzawiBelum ada peringkat
- Educ 205 Special Education Final 2022Dokumen1 halamanEduc 205 Special Education Final 2022Eduardo CasesBelum ada peringkat
- Test Bank For Social Studies in Elementary Education Plus Myeducationlab With Pearson Etext Access Card Package 14 e 14th EditionDokumen38 halamanTest Bank For Social Studies in Elementary Education Plus Myeducationlab With Pearson Etext Access Card Package 14 e 14th Editionbhangglassilyihpok100% (8)
- Teaching Strategies Based On Multiple Intelligences Theory Among Science and Mathematics Secondary School TeachersDokumen7 halamanTeaching Strategies Based On Multiple Intelligences Theory Among Science and Mathematics Secondary School TeachersjeckBelum ada peringkat
- Skripsi Learning StyleDokumen256 halamanSkripsi Learning StyleAnsor PutraBelum ada peringkat
- Project Report Format-1Dokumen11 halamanProject Report Format-1Deepti Singh KashyapBelum ada peringkat
- Drama Teaching and Learning SyllabusDokumen26 halamanDrama Teaching and Learning SyllabusAndrei Cristian AnghelBelum ada peringkat
- The Teacher as a CurricularistDokumen3 halamanThe Teacher as a CurricularistEricka Shane EspejoBelum ada peringkat
- Anderson & Otalora - 2010 - Designing A Course On CLIL For In-Service Teacher Education PDFDokumen32 halamanAnderson & Otalora - 2010 - Designing A Course On CLIL For In-Service Teacher Education PDFcarlazBelum ada peringkat
- Group 2 ResearchDokumen22 halamanGroup 2 ResearchKeithfrancis LaparanBelum ada peringkat
- Teacher Student Assessment SheetDokumen7 halamanTeacher Student Assessment SheetBearys GroupBelum ada peringkat
- DCSS Acr NRMDokumen13 halamanDCSS Acr NRMMae Ann Villar CadungganBelum ada peringkat
- AS and A Level: ChemistryDokumen11 halamanAS and A Level: ChemistryStingy BieBelum ada peringkat
- Lesson Plan 1 - What Do Seeds Need To Grow Group 1Dokumen5 halamanLesson Plan 1 - What Do Seeds Need To Grow Group 1api-321143976Belum ada peringkat
- EMPS 311EDUCATIONAL PLANNINGNOTES - Edited-1Dokumen57 halamanEMPS 311EDUCATIONAL PLANNINGNOTES - Edited-1austinoyugi08Belum ada peringkat
- (APCEIU) 2022 APTW Concept Note - CompDokumen4 halaman(APCEIU) 2022 APTW Concept Note - CompMelanie CortezBelum ada peringkat