Anda mungkin juga menyukai
- NCP AgeDokumen1 halamanNCP AgecaressmeBelum ada peringkat
- Renal Failure NCPDokumen3 halamanRenal Failure NCPjsksBelum ada peringkat
- Assessment Diagnosis Planning Implementation Rationale EvaluationDokumen14 halamanAssessment Diagnosis Planning Implementation Rationale EvaluationJennifer ArdeBelum ada peringkat
- NcpsDokumen10 halamanNcpskotoirBelum ada peringkat
- NCP and DStudyDokumen8 halamanNCP and DStudyJessica Rosan Hewald ManapatBelum ada peringkat
- FractureDokumen4 halamanFractureRaveen mayiBelum ada peringkat
- Incomplete Spinal Cord Injury Nursing CareDokumen6 halamanIncomplete Spinal Cord Injury Nursing CareTherese MargaretBelum ada peringkat
- NCP PainDokumen2 halamanNCP PainApril_Ivy_Raga_3835Belum ada peringkat
- NCP CKDDokumen3 halamanNCP CKDRiel TumandaBelum ada peringkat
- NCP Ineffective Cardiopulmonary PerfusionDokumen3 halamanNCP Ineffective Cardiopulmonary PerfusionjamiemapanaoBelum ada peringkat
- Nursing Care Plans For Activity IntoleranceDokumen4 halamanNursing Care Plans For Activity IntolerancethebigtwirpBelum ada peringkat
- NCP Sa Sinus Tachycardia FinalDokumen13 halamanNCP Sa Sinus Tachycardia FinalMYKRISTIE JHO MENDEZBelum ada peringkat
- Healthcare - Nursing Care Plan - Excess Fluid VolumeDokumen4 halamanHealthcare - Nursing Care Plan - Excess Fluid VolumeBenjamin CañalitaBelum ada peringkat
- SLCN Gazette Magazine, Volume 1, Issue 1, 2019Dokumen20 halamanSLCN Gazette Magazine, Volume 1, Issue 1, 2019Mayzelle RizBelum ada peringkat
- NCP On DyspneaDokumen5 halamanNCP On DyspneaDizzy BualanBelum ada peringkat
- Nursing Responsibilities For Oxygen AdministrationDokumen3 halamanNursing Responsibilities For Oxygen AdministrationJahseh WolfeBelum ada peringkat
- NCP-Case Presentation (CHF)Dokumen4 halamanNCP-Case Presentation (CHF)Jessamine EnriquezBelum ada peringkat
- AmiodaroneDokumen2 halamanAmiodaroneanindiawBelum ada peringkat
- NCP Knowledge Deficit PDFDokumen2 halamanNCP Knowledge Deficit PDFskylertBelum ada peringkat
- NCPDokumen6 halamanNCPBelle OyosBelum ada peringkat
- Terazosin Hydro ChlorideDokumen3 halamanTerazosin Hydro Chlorideapi-3797941Belum ada peringkat
- NCP Self CaRE DeficitDokumen1 halamanNCP Self CaRE Deficitnicole pageBelum ada peringkat
- Code Green Introduction Reviewer - RedDokumen4 halamanCode Green Introduction Reviewer - RedJamieBelum ada peringkat
- NCPDokumen3 halamanNCPErica Denice CastilloBelum ada peringkat
- Nursing Care Plan for Post-Surgical PainDokumen3 halamanNursing Care Plan for Post-Surgical PainAngelgodess Athena-envyBelum ada peringkat
- LortabDokumen1 halamanLortabSheri490Belum ada peringkat
- NCP Decreased Cardiac Output 1Dokumen2 halamanNCP Decreased Cardiac Output 1Arnel MacabalitaoBelum ada peringkat
- Assess For Signs of HyperglycemiaDokumen9 halamanAssess For Signs of HyperglycemiaSheril Sularte CasanesBelum ada peringkat
- Hyperthyroidism Nursing Care Plans - 7 Common NCPsDokumen1 halamanHyperthyroidism Nursing Care Plans - 7 Common NCPsApol PenBelum ada peringkat
- Types of Definitions ExerciseDokumen2 halamanTypes of Definitions ExerciseDaniella TimbolBelum ada peringkat
- DX Fracture PDFDokumen8 halamanDX Fracture PDFSherree HayesBelum ada peringkat
- Reaction Paper ERDokumen1 halamanReaction Paper ERVann Anthony FuentesBelum ada peringkat
- NCM 114 - NCPDokumen3 halamanNCM 114 - NCPReysiela Mae ValinoBelum ada peringkat
- NCP Proper CholecystectomyDokumen2 halamanNCP Proper CholecystectomyGail Lian SantosBelum ada peringkat
- Nursing Care Plan for Diabetic Patient with DehydrationDokumen2 halamanNursing Care Plan for Diabetic Patient with DehydrationRodolfo Bong SemaneroBelum ada peringkat
- Sample CHN Teaching Learning GuideDokumen3 halamanSample CHN Teaching Learning GuideSUREEN MAY ANG REGULARBelum ada peringkat
- Case 1Dokumen9 halamanCase 1Joselyn M. LachicaBelum ada peringkat
- Head Nurse: General ObjectiveDokumen10 halamanHead Nurse: General Objectiveeihjay-bravo-8041Belum ada peringkat
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDokumen8 halamanNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiBelum ada peringkat
- Disturbed Sleep PatternDokumen1 halamanDisturbed Sleep PatternHsintan HsuBelum ada peringkat
- Emj Cases : Questions For Case 1Dokumen8 halamanEmj Cases : Questions For Case 1Azmyza Azmy100% (1)
- NURSING CARE PLAN FOR POSTPARTUM HEMORRHAGEDokumen3 halamanNURSING CARE PLAN FOR POSTPARTUM HEMORRHAGEKrizzy Chen100% (1)
- Group 9 Sickle Cell Anemia Case Study ActivityDokumen4 halamanGroup 9 Sickle Cell Anemia Case Study ActivityJuliaBelum ada peringkat
- Impaired Skin IntegrityDokumen3 halamanImpaired Skin IntegrityAubrey SungaBelum ada peringkat
- Novilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationDokumen1 halamanNovilyn C. Pataray BSN - Ii: Assessment Diagnosi S Pathophysiolog Y Planning Interevention Rationale EvaluationCharina AubreyBelum ada peringkat
- NCPDokumen3 halamanNCPJezza RequilmeBelum ada peringkat
- Heart Perfusion Nursing CareDokumen12 halamanHeart Perfusion Nursing CareSesinando Niez Quilao Jr.100% (1)
- Managing Fatigue Through Activity Pacing and RestDokumen2 halamanManaging Fatigue Through Activity Pacing and ResthaniehaehaeBelum ada peringkat
- Written Report:: Transitional Human ShelterDokumen7 halamanWritten Report:: Transitional Human ShelterKasandra Dawn Moquia BerisoBelum ada peringkat
- Hypertension Related To Faulty Eating Habits As Evidence My Blood Pressure of 13080.Dokumen2 halamanHypertension Related To Faulty Eating Habits As Evidence My Blood Pressure of 13080.Senyorita KHayeBelum ada peringkat
- NCP Knowledge DeficitDokumen2 halamanNCP Knowledge DeficitPrincess Faniega SugatonBelum ada peringkat
- Week 3. COURSE TASK - Acute PancreatitisDokumen3 halamanWeek 3. COURSE TASK - Acute PancreatitisqwertBelum ada peringkat
- NCP EsrfDokumen9 halamanNCP EsrfKen RegalaBelum ada peringkat
- Mosegor Vita Is A Vitamin SupplementDokumen1 halamanMosegor Vita Is A Vitamin SupplementlolabayBelum ada peringkat
- Angiotensin Converting Enzyme (ACE) InhibitorsDokumen4 halamanAngiotensin Converting Enzyme (ACE) InhibitorsPutri Mulia HasibuanBelum ada peringkat
- E. Nursing DiagnosisDokumen2 halamanE. Nursing DiagnosisAle SandraBelum ada peringkat
- Altered Renal Perfusion CRFDokumen4 halamanAltered Renal Perfusion CRFKristel Anne Nillo ZepolBelum ada peringkat
- Mrs. MM Nursing Care PlanDokumen34 halamanMrs. MM Nursing Care PlanIsobel Mae JacelaBelum ada peringkat
- Diagnosa Baru EinDokumen2 halamanDiagnosa Baru EinthethayBelum ada peringkat
- NCP For Imbalanced NutritionDokumen6 halamanNCP For Imbalanced NutritionMelvin MartinezBelum ada peringkat
- 4 Revised Worksheet Template August8,2014Dokumen7 halaman4 Revised Worksheet Template August8,2014Mary Gold EleveraBelum ada peringkat
- Captivate UsDokumen2 halamanCaptivate UsMary Gold EleveraBelum ada peringkat
- School FormsDokumen18 halamanSchool FormsChariza Lumain AlcazarBelum ada peringkat
- SDGs BookletDokumen21 halamanSDGs BookletFabolos 9Belum ada peringkat
- 20120221Dokumen2 halaman20120221Mary Gold EleveraBelum ada peringkat
- SDGs BookletDokumen21 halamanSDGs BookletFabolos 9Belum ada peringkat
- Ncbts PDFDokumen41 halamanNcbts PDFRose de DiosBelum ada peringkat
- AssessmentforLearning PDFDokumen49 halamanAssessmentforLearning PDFwolfvor0% (1)
- PHADokumen17 halamanPHAMary Gold EleveraBelum ada peringkat
- CS Form No. 212 Revised Personal Data Sheet Sample FormDokumen16 halamanCS Form No. 212 Revised Personal Data Sheet Sample Formpinoycashminero78% (150)
- 10-Point Socioeconomic Agenda of The Duterte Administration: Dr. Paulyn Jean B. Rosell-UbialDokumen5 halaman10-Point Socioeconomic Agenda of The Duterte Administration: Dr. Paulyn Jean B. Rosell-UbialMary Gold EleveraBelum ada peringkat
- January Date: National Blood Donors MonthDokumen14 halamanJanuary Date: National Blood Donors MonthMary Gold EleveraBelum ada peringkat
- Computer LessonDokumen1 halamanComputer LessonMary Gold EleveraBelum ada peringkat
- QUOTES About Loving YourselfDokumen25 halamanQUOTES About Loving YourselfMary Gold EleveraBelum ada peringkat
- ER Journals For Duty Mar5-8,2012Dokumen3 halamanER Journals For Duty Mar5-8,2012Mary Gold EleveraBelum ada peringkat
- Dessert RecipesDokumen6 halamanDessert RecipesMary Gold EleveraBelum ada peringkat
- Maximizing Growth Factors for Height IncreaseDokumen29 halamanMaximizing Growth Factors for Height IncreaseMegaV100% (2)
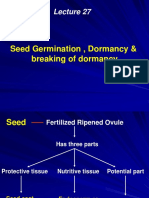
- Seed Germination, Dormancy & Breaking of DormancyDokumen35 halamanSeed Germination, Dormancy & Breaking of DormancySaravananBelum ada peringkat
- Uji Aktivitas Antioksidan Ekstrak Etanol 70% Bunga Telang (Clitoria TernateaL) Dari Daerah Sleman Dengan Metode DPPHDokumen7 halamanUji Aktivitas Antioksidan Ekstrak Etanol 70% Bunga Telang (Clitoria TernateaL) Dari Daerah Sleman Dengan Metode DPPHAnastasia FebruestiBelum ada peringkat
- Altered Body TemperatureDokumen27 halamanAltered Body TemperatureAnusikta PandaBelum ada peringkat
- How Sleeping Positions Impact Sleep Quality and HealthDokumen2 halamanHow Sleeping Positions Impact Sleep Quality and HealthNeelesh Suteri0% (1)
- Battle of BrainDokumen7 halamanBattle of BrainKhalida Zia SiregarBelum ada peringkat
- LAB EXERCISE 1 Organization of The Human BodyDokumen8 halamanLAB EXERCISE 1 Organization of The Human Bodyley leynBelum ada peringkat
- Science: Quarter 1 - Module 1Dokumen10 halamanScience: Quarter 1 - Module 1RUTH PIANGBelum ada peringkat
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDokumen8 halamanTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaBelum ada peringkat
- CBSE Quick Revision Notes on Mineral NutritionDokumen5 halamanCBSE Quick Revision Notes on Mineral NutritionTushar RajBelum ada peringkat
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDokumen14 halamanOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhBelum ada peringkat
- Chapter 4Dokumen7 halamanChapter 4R LashBelum ada peringkat
- Fetal Circulation (For MBBS)Dokumen50 halamanFetal Circulation (For MBBS)Tashif100% (1)
- General Zoology SyllabusDokumen4 halamanGeneral Zoology SyllabusNL R Q DO100% (3)
- Neurodegenerative Cerebellar AtaxiaDokumen26 halamanNeurodegenerative Cerebellar AtaxiaМилица МилошевићBelum ada peringkat
- Abdominal SurgeryDokumen166 halamanAbdominal SurgeryIndera VyasBelum ada peringkat
- Amino Acid Sequences Reveal Evolutionary RelationshipsDokumen6 halamanAmino Acid Sequences Reveal Evolutionary RelationshipsAbby Gail DigalBelum ada peringkat
- Anatomy and Physiology TermsDokumen8 halamanAnatomy and Physiology TermsDominic DinioBelum ada peringkat
- Vacuole FunctionDokumen8 halamanVacuole Functionkbansal981Belum ada peringkat
- Top Knife - Cutted - Top PDFDokumen238 halamanTop Knife - Cutted - Top PDFIvanKazaiev100% (1)
- CHAPTER SUMMARY-opiod AnalgesicDokumen9 halamanCHAPTER SUMMARY-opiod AnalgesicNuttiya WerawattanachaiBelum ada peringkat
- 201305283en Capsurefix 5076Dokumen2 halaman201305283en Capsurefix 5076Bian PurwaBelum ada peringkat
- Risk For Decreased Cardiac OutputDokumen4 halamanRisk For Decreased Cardiac Outputapi-283482759Belum ada peringkat
- Mitosis and MeiosisDokumen4 halamanMitosis and MeiosisMicah Porcal ArelladoBelum ada peringkat
- The Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Dokumen10 halamanThe Third International Consensus Definitions For Sepsis and Septic Shock Sepsis-3 - JAMA 2016Miguel Angel Quiroz CristobalBelum ada peringkat
- Drug StudyDokumen11 halamanDrug StudyKimberly Ann MendozaBelum ada peringkat
- Tetanus Neonatorum LectureDokumen11 halamanTetanus Neonatorum LectureJackBelum ada peringkat
- Brainstem Bravo AnnotatedDokumen13 halamanBrainstem Bravo AnnotatedMia CadizBelum ada peringkat
- Test Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendDokumen15 halamanTest Bank For Essentials of Psychiatric Mental Health Nursing 7th Edition Mary C TownsendVanessa Martin100% (30)
- ReadingsDokumen246 halamanReadingsFul WgBelum ada peringkat