Anda mungkin juga menyukai
- MMPDokumen12 halamanMMPANIS MURNIATIBelum ada peringkat
- 1017 FullDokumen11 halaman1017 FullANIS MURNIATIBelum ada peringkat
- Phenotypic Stability of Articular Chondrocytes in VitroDokumen9 halamanPhenotypic Stability of Articular Chondrocytes in VitroANIS MURNIATIBelum ada peringkat
- 2-4 Paper3Dokumen9 halaman2-4 Paper3ANIS MURNIATIBelum ada peringkat
- 23.correlation of Plasma and Synovial Fluid Adiponectin With Knee Osteoarthritis SeverityDokumen6 halaman23.correlation of Plasma and Synovial Fluid Adiponectin With Knee Osteoarthritis SeverityANIS MURNIATIBelum ada peringkat
- 2010 SteinhagenDokumen7 halaman2010 SteinhagenANIS MURNIATIBelum ada peringkat
- S1063458412X00116 S1063458412008710 MainDokumen9 halamanS1063458412X00116 S1063458412008710 MainANIS MURNIATIBelum ada peringkat
- Cell Cycle in NeuronsDokumen11 halamanCell Cycle in NeuronsJulian AlejandroBelum ada peringkat
- Enhancing Post-Expansion Chondrogenic Potential of Costochondral Cells in Self-Assembled NeocartilageDokumen10 halamanEnhancing Post-Expansion Chondrogenic Potential of Costochondral Cells in Self-Assembled NeocartilageANIS MURNIATIBelum ada peringkat
- 286Dokumen10 halaman286ANIS MURNIATIBelum ada peringkat
- 2 7Dokumen13 halaman2 7ANIS MURNIATIBelum ada peringkat
- Ar 2181Dokumen9 halamanAr 2181ANIS MURNIATIBelum ada peringkat
- In Vitro Engineering of Human Autogenous Cartilage: Ursula Anderer and Jeanette LiberaDokumen10 halamanIn Vitro Engineering of Human Autogenous Cartilage: Ursula Anderer and Jeanette LiberaANIS MURNIATIBelum ada peringkat
- Phenotypic Stability of Articular Chondrocytes in VitroDokumen9 halamanPhenotypic Stability of Articular Chondrocytes in VitroANIS MURNIATIBelum ada peringkat
- Ujian SMP 2 My VersionDokumen13 halamanUjian SMP 2 My VersionANIS MURNIATIBelum ada peringkat
- ArthritisDokumen9 halamanArthritisANIS MURNIATIBelum ada peringkat
- Prestasi Application Form 2013Dokumen29 halamanPrestasi Application Form 2013Rahmat HidayatBelum ada peringkat
- Praktikum Spektro RegulerDokumen2 halamanPraktikum Spektro RegulerANIS MURNIATIBelum ada peringkat
- Hum. Reprod.-2006-García-Pérez-880-7Dokumen8 halamanHum. Reprod.-2006-García-Pérez-880-7ANIS MURNIATIBelum ada peringkat
- Primary OsteoarthritisDokumen1 halamanPrimary OsteoarthritisANIS MURNIATIBelum ada peringkat
- Coronary Artery DiseaseDokumen5 halamanCoronary Artery DiseaseANIS MURNIATIBelum ada peringkat
- The CNS Regulates The Immune System Through Two Major MechanismsDokumen1 halamanThe CNS Regulates The Immune System Through Two Major MechanismsANIS MURNIATIBelum ada peringkat
- The CNS Regulates The Immune System Through Two Major MechanismsDokumen1 halamanThe CNS Regulates The Immune System Through Two Major MechanismsANIS MURNIATIBelum ada peringkat
- Peran Vitamin D Dalam Regulasi Sistem Imunitas Melalui Sel Dendritik Oleh Wira DaramatasiaDokumen2 halamanPeran Vitamin D Dalam Regulasi Sistem Imunitas Melalui Sel Dendritik Oleh Wira DaramatasiaANIS MURNIATIBelum ada peringkat
- Coronary Artery DiseaseDokumen5 halamanCoronary Artery DiseaseANIS MURNIATIBelum ada peringkat
- Long Live Th2Dokumen18 halamanLong Live Th2ANIS MURNIATIBelum ada peringkat
- Dna Repair PDFDokumen8 halamanDna Repair PDFANIS MURNIATIBelum ada peringkat
- The Most Important Factor in Predicting Prognosis in AML Is The Genetic MakeDokumen1 halamanThe Most Important Factor in Predicting Prognosis in AML Is The Genetic MakeANIS MURNIATIBelum ada peringkat
- Silabus Mata Kuliah Patobilologi KankerDokumen2 halamanSilabus Mata Kuliah Patobilologi KankerANIS MURNIATIBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Jurnal CA RektiDokumen8 halamanJurnal CA RektiIvan HoBelum ada peringkat
- 13 Surprising Benefits of Papaya (Pawpaw) - Organic FactsDokumen10 halaman13 Surprising Benefits of Papaya (Pawpaw) - Organic FactsStela GallarBelum ada peringkat
- Pancreatic Solid LeasionsDokumen24 halamanPancreatic Solid LeasionsEliza CrăciunBelum ada peringkat
- Cancer Immunotherapy ReviewDokumen10 halamanCancer Immunotherapy ReviewNenad MladenovicBelum ada peringkat
- Four pillars of healthy living reduce NCD riskDokumen5 halamanFour pillars of healthy living reduce NCD riskLea TanBelum ada peringkat
- NHLBI - Anemia - Infographic - v06 - RELEASE 508Dokumen1 halamanNHLBI - Anemia - Infographic - v06 - RELEASE 508bnvjBelum ada peringkat
- Dhikr Therapy For Reducing Anxiety in Cancer PatientDokumen6 halamanDhikr Therapy For Reducing Anxiety in Cancer PatientRisfialdo Lily WidiatamaBelum ada peringkat
- Oncology NursingDokumen12 halamanOncology NursingDick Morgan Ferrer80% (5)
- Anaplastic Sarcoma of The Kidney With Chromosomal AbnormalityDokumen5 halamanAnaplastic Sarcoma of The Kidney With Chromosomal AbnormalityJose Alejandro InciongBelum ada peringkat
- AJCC Cancer Staging Form Supplement PDFDokumen514 halamanAJCC Cancer Staging Form Supplement PDFSaint Germain Valencia RondónBelum ada peringkat
- Concept Map Case Study E2Dokumen5 halamanConcept Map Case Study E2api-283004290Belum ada peringkat
- Testimonies of Crimes Against Humanity in FallujahDokumen32 halamanTestimonies of Crimes Against Humanity in Fallujahpaola pisiBelum ada peringkat
- New Development of Ashitaba Canton 2Dokumen23 halamanNew Development of Ashitaba Canton 2Angel John Fofue JalopBelum ada peringkat
- Breast Cancer Risk Assessment by Gail Model in Women of Baghdad PDFDokumen4 halamanBreast Cancer Risk Assessment by Gail Model in Women of Baghdad PDFSalam H AlhelaliBelum ada peringkat
- Modified Radical MastectomyDokumen6 halamanModified Radical Mastectomymetch isulatBelum ada peringkat
- GL Medic Surv 2001 PDFDokumen139 halamanGL Medic Surv 2001 PDFAlief AzizBelum ada peringkat
- No. No. of MCQ 'SDokumen16 halamanNo. No. of MCQ 'SUddhav KumbharBelum ada peringkat
- TobaccoDokumen274 halamanTobaccoPat ChompumingBelum ada peringkat
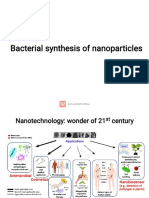
- Bacterial Synthesis of Nanoparticles for Biomedical ApplicationsDokumen16 halamanBacterial Synthesis of Nanoparticles for Biomedical ApplicationsDibyajyoti20 Das4001Belum ada peringkat
- Antiemesis NCCNDokumen79 halamanAntiemesis NCCNana salazarBelum ada peringkat
- PSMADokumen10 halamanPSMADiego GavilanesBelum ada peringkat
- First Aid 2015 Pages AddedDokumen11 halamanFirst Aid 2015 Pages AddedNicole WilliamBelum ada peringkat
- Video Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaDokumen1 halamanVideo Conten - 2017 - Blumgart S Surgery of The Liver Biliary Tract and PancreaJoe JoeBelum ada peringkat
- ONC1119 Ezine PDFDokumen48 halamanONC1119 Ezine PDFdanishBelum ada peringkat
- The Impact of Physical Activities On The Health of AdultsDokumen12 halamanThe Impact of Physical Activities On The Health of AdultsJUNAID AHMEDBelum ada peringkat
- Etiology of Optic Atrophy in Saudi ArabiaDokumen8 halamanEtiology of Optic Atrophy in Saudi ArabiaStar LadyBelum ada peringkat
- On LeukemiaDokumen28 halamanOn LeukemiaMeena Koushal100% (1)
- Molecular Oncology: Directory of ServicesDokumen31 halamanMolecular Oncology: Directory of Servicesruby_kakkar9796100% (2)
- Antimicrobial Mikania MicranthaDokumen11 halamanAntimicrobial Mikania MicranthaArchrys Mia LicyayoBelum ada peringkat
- AnanthDokumen85 halamanAnanthFahad iqbalBelum ada peringkat