Anda mungkin juga menyukai
- Pereira 2015Dokumen9 halamanPereira 2015Amalia RosaBelum ada peringkat
- The Prevalence of in The Knee Osteoarthritis ElderlyDokumen5 halamanThe Prevalence of in The Knee Osteoarthritis Elderlyqurrat ul ann haiderBelum ada peringkat
- Association Between Knee Osteoarthritis and Volumetric Bone Mineral DensityDokumen14 halamanAssociation Between Knee Osteoarthritis and Volumetric Bone Mineral Densitytranminhtri21062001Belum ada peringkat
- 2009 Article 957Dokumen8 halaman2009 Article 957Firda PotterBelum ada peringkat
- Movement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDokumen10 halamanMovement Detection Impaired in Patients With Knee Osteoarthritis Compared To Healthy Controls: A Cross-Sectional Case-Control StudyDavid SugiartoBelum ada peringkat
- Does Osteoporosis Increase Early Subsidence of Cementless Double-Tapered Femoral Stem in Hip Arthroplasty?Dokumen5 halamanDoes Osteoporosis Increase Early Subsidence of Cementless Double-Tapered Femoral Stem in Hip Arthroplasty?LuisAngelPonceTorresBelum ada peringkat
- Issue 21Dokumen9 halamanIssue 21Abuzdea AlexBelum ada peringkat
- Associations of Radiological Osteoarthritis of The Hip and Knee With Locomotor Disability in The Rotterdam StudyDokumen6 halamanAssociations of Radiological Osteoarthritis of The Hip and Knee With Locomotor Disability in The Rotterdam StudyRebecca CooperBelum ada peringkat
- MRI, Força de ExtensoresDokumen16 halamanMRI, Força de ExtensoresRosaneLacerdaBelum ada peringkat
- Mito, Mitani SatoDokumen6 halamanMito, Mitani SatoNarcisa Lamilla Jimenez de RamosBelum ada peringkat
- Epidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangDokumen19 halamanEpidemiologyofosteoarthritis: Tuhina Neogi,, Yuqing ZhangIkmal ShahromBelum ada peringkat
- Good Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Dokumen183 halamanGood Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Ary MfBelum ada peringkat
- Reliability of Growth Prediction With Hand - Wrist RadiographsDokumen5 halamanReliability of Growth Prediction With Hand - Wrist Radiographscalmua1234Belum ada peringkat
- Residual Hip Dysplasia As A Risk Factor For Osteoarthritis in 45 Years Follow-Up of Late-Detected Hip DislocatioDokumen7 halamanResidual Hip Dysplasia As A Risk Factor For Osteoarthritis in 45 Years Follow-Up of Late-Detected Hip DislocatioManolis MorakisBelum ada peringkat
- Nice 1stDokumen6 halamanNice 1staldiBelum ada peringkat
- Cadera 01Dokumen6 halamanCadera 01Jordi ArlandisBelum ada peringkat
- Characteristics and Severity of Osteoarthritis Among Patients in Mogadishu Somalia: A Single Center Cross-Sectional StudyDokumen9 halamanCharacteristics and Severity of Osteoarthritis Among Patients in Mogadishu Somalia: A Single Center Cross-Sectional StudyIJAR JOURNALBelum ada peringkat
- Hamstring Length in Patellofemoral Pain Syndrome: Lisa C. White, Philippa Dolphin, John DixonDokumen5 halamanHamstring Length in Patellofemoral Pain Syndrome: Lisa C. White, Philippa Dolphin, John DixonMamedBelum ada peringkat
- Gambaran Kejadian Nyeri Lutut Dengan Kecurigaan Osteoartritis Lutut Pada Perawat Di Poliklinik Rawat Jalan Blu Rsup. Prof. Dr. R. D. Kandou ManadoDokumen5 halamanGambaran Kejadian Nyeri Lutut Dengan Kecurigaan Osteoartritis Lutut Pada Perawat Di Poliklinik Rawat Jalan Blu Rsup. Prof. Dr. R. D. Kandou ManadochitraBelum ada peringkat
- A Prospective Study of Efficacy and Outcome Analysis of Role of PRP Injection in Osteoarthritis of Knee Joint 40 Cases Prospective AnalysisDokumen6 halamanA Prospective Study of Efficacy and Outcome Analysis of Role of PRP Injection in Osteoarthritis of Knee Joint 40 Cases Prospective AnalysisIJAR JOURNALBelum ada peringkat
- Assessment of Skeletal Maturity of The Hand-Wrist and Knee: A Comparison Among MethodsDokumen6 halamanAssessment of Skeletal Maturity of The Hand-Wrist and Knee: A Comparison Among MethodsJoBelum ada peringkat
- Relationship Between Knee and Ankle Degeneration in A Population of Organ DonorsDokumen11 halamanRelationship Between Knee and Ankle Degeneration in A Population of Organ DonorsNguyễn HùngBelum ada peringkat
- Comparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodDokumen5 halamanComparing The Effects of Ultrasound and Microwave Physiotherapy Treatments On Knee Osteoarthritis by MEasuring Osteocalcin Level and Erythrocyte Sedimentation Rate in BloodAlfiana ApriliaBelum ada peringkat
- InTech-Knee Pain in Adults Adolescents Diagnosis and TreatmentDokumen32 halamanInTech-Knee Pain in Adults Adolescents Diagnosis and Treatmentevil freakBelum ada peringkat
- Gastritis 1Dokumen5 halamanGastritis 1IttyBelum ada peringkat
- Effect of Rheumatoid Arthritis On Primary Total Knee Arthroplasty and Revision ArthroplastyDokumen6 halamanEffect of Rheumatoid Arthritis On Primary Total Knee Arthroplasty and Revision Arthroplasty송성욱Belum ada peringkat
- First Carpometacarpal and InteDokumen6 halamanFirst Carpometacarpal and InteStephanie Mhae TabasaBelum ada peringkat
- Tennis Elbow JOSPT ArticleDokumen11 halamanTennis Elbow JOSPT ArticleHasan RahmanBelum ada peringkat
- PTJ/PZZ 182Dokumen24 halamanPTJ/PZZ 182leticia coutinhoBelum ada peringkat
- Incidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDokumen5 halamanIncidental Findings of The Lumbar Spine at MRI During Herniated Intervertebral Disk Disease EvaluationDyah Gaby KesumaBelum ada peringkat
- Ymj 59 317Dokumen8 halamanYmj 59 317ItaloLozanoPalominoBelum ada peringkat
- Does Standing Protect Bone Density in Patients WithDokumen5 halamanDoes Standing Protect Bone Density in Patients WithManos AndriolasBelum ada peringkat
- RX Utiles DCDDokumen4 halamanRX Utiles DCDAlicia BallesterosBelum ada peringkat
- 6 Brief Resume of Intended Work 6.1 Need For The StudyDokumen12 halaman6 Brief Resume of Intended Work 6.1 Need For The StudyFerrdy Pratama WBelum ada peringkat
- Original ArticleDokumen7 halamanOriginal ArticleFirdaus Septhy ArdhyanBelum ada peringkat
- tmp9968 TMPDokumen3 halamantmp9968 TMPFrontiersBelum ada peringkat
- Knee Osteoarthritis Assessment Management Presentation SlidesDokumen304 halamanKnee Osteoarthritis Assessment Management Presentation SlidesMuhammad Tahir50% (2)
- Outcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or YoungerDokumen8 halamanOutcomes of Hip Arthroscopy in Patients Aged 50 Years or Older Compared With A Matched-Pair Control of Patients Aged 30 Years or Youngersuad5stambulieBelum ada peringkat
- 2016 Article 171Dokumen5 halaman2016 Article 171arvinelaBelum ada peringkat
- Risk Factors and Burden of Osteoarthritis: SciencedirectDokumen5 halamanRisk Factors and Burden of Osteoarthritis: SciencedirectlindapramusintaBelum ada peringkat
- The Relation of Q Angle and Anthropometric Measures With Ankle Sprain A Case-Control StudyDokumen4 halamanThe Relation of Q Angle and Anthropometric Measures With Ankle Sprain A Case-Control StudyyohanesBelum ada peringkat
- 1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsDokumen8 halaman1756-185X.13082) Huang, Lanfeng Guo, Bin Xu, Feixiang Zhao, Jinsong - Effects of Quadriceps Functional Exercise With IsTrisna ArinataBelum ada peringkat
- Research Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?Dokumen8 halamanResearch Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?gloriagaskBelum ada peringkat
- Characteristics of Morphometric Parameters of Children With ScoliosisDokumen4 halamanCharacteristics of Morphometric Parameters of Children With ScoliosisOpen Access JournalBelum ada peringkat
- Association of Pars Defect Type With Clinical Outcome After Smiley Face Rod Methods For Terminal-Stage SpondylolysisDokumen8 halamanAssociation of Pars Defect Type With Clinical Outcome After Smiley Face Rod Methods For Terminal-Stage SpondylolysisUzm.Dr.Burhan ORAL GÜDÜBelum ada peringkat
- Research Article: Predictions of The Length of Lumbar Puncture NeedlesDokumen5 halamanResearch Article: Predictions of The Length of Lumbar Puncture NeedlesNefri ArshintaBelum ada peringkat
- Knee Osteoarthritis Patient 5Dokumen8 halamanKnee Osteoarthritis Patient 5TanvirBelum ada peringkat
- Evaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramDokumen13 halamanEvaluation of The Lateral Instability of The Ankle by Inversion Simulation Device and Assessment of The Rehabilitation ProgramZzDel VerdeBelum ada peringkat
- Conclusions 2000 - Jurnal - Effects of Ethnicity On Skeletal Maturation: Consequences For Forensic Age EstimationsDokumen4 halamanConclusions 2000 - Jurnal - Effects of Ethnicity On Skeletal Maturation: Consequences For Forensic Age EstimationsTiara LioBelum ada peringkat
- FulltextDokumen11 halamanFulltextajeet84bhu2920Belum ada peringkat
- Diabetes and Risk of Fracture: The Blue Mountains Eye StudyDokumen6 halamanDiabetes and Risk of Fracture: The Blue Mountains Eye Studymuhammad subhanBelum ada peringkat
- Vertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenDokumen11 halamanVertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenAdhiatma DotBelum ada peringkat
- Avascular Necrosis As A Complication of The Treatment of Dislocation of The Hip in Children With Cerebral PalsyDokumen7 halamanAvascular Necrosis As A Complication of The Treatment of Dislocation of The Hip in Children With Cerebral PalsyDeepak NemaniBelum ada peringkat
- Radiologic Evaluation of The Distal Radius Indices in Early and Late ChildhoodDokumen4 halamanRadiologic Evaluation of The Distal Radius Indices in Early and Late ChildhoodRafaelAntonioNarvaezAguirreBelum ada peringkat
- Genu Valgum and Flat Feet in Children With Healthy.15Dokumen7 halamanGenu Valgum and Flat Feet in Children With Healthy.15saarita lozano piedraBelum ada peringkat
- AnnNuclMedSci05!18!143 (3 Huang)Dokumen6 halamanAnnNuclMedSci05!18!143 (3 Huang)Harun NasutionBelum ada peringkat
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDokumen4 halamanSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraBelum ada peringkat
- Influence of High-Heeled Shoes On The Sagittal Balance of The Spine and The Whole Body 2016 PDFDokumen8 halamanInfluence of High-Heeled Shoes On The Sagittal Balance of The Spine and The Whole Body 2016 PDFJuan Carlos LescanoBelum ada peringkat
- Comparison of Clinical Severity of Congenital Muscular Torticollis Based On The Method of Child BirthDokumen12 halamanComparison of Clinical Severity of Congenital Muscular Torticollis Based On The Method of Child BirthBia SafitriBelum ada peringkat
- Flower Arrangement: Tulip: © Canon Inc. © MinyaDokumen4 halamanFlower Arrangement: Tulip: © Canon Inc. © MinyaFranchesca OrtizBelum ada peringkat
- Sarcopenic Obesity Predicts Instrumental Activities of Daily Living Disability in The ElderlyDokumen10 halamanSarcopenic Obesity Predicts Instrumental Activities of Daily Living Disability in The ElderlyFranchesca OrtizBelum ada peringkat
- Surgical Management of Adolescent Varicocele Systematic Review of The World LiteratureDokumen7 halamanSurgical Management of Adolescent Varicocele Systematic Review of The World LiteratureFranchesca OrtizBelum ada peringkat
- Pectus Excavatum and Hereditable Disorders of The Connective TissueDokumen6 halamanPectus Excavatum and Hereditable Disorders of The Connective TissueFranchesca Ortiz100% (1)
- Coronary Artery Involvement in PediatricDokumen5 halamanCoronary Artery Involvement in PediatricFranchesca OrtizBelum ada peringkat
- Central Precocious PubertyDokumen3 halamanCentral Precocious PubertyFranchesca OrtizBelum ada peringkat
- Foot Ankle Spec 2013 KarimiDokumen7 halamanFoot Ankle Spec 2013 KarimiFranchesca OrtizBelum ada peringkat
- Importance and Challenges of Measuring IntrinsicDokumen14 halamanImportance and Challenges of Measuring IntrinsicFranchesca OrtizBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaSyaidyHamdanBelum ada peringkat
- Cranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Dokumen262 halamanCranial Nerves - Function and Dysfunctions, 3E (2010) (PDF) (UnitedVRG)Alvaro RivCalle87% (15)
- Knowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonDokumen7 halamanKnowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonNadira Juanti PratiwiBelum ada peringkat
- Arterial Blood Gas Values Case Study 2Dokumen3 halamanArterial Blood Gas Values Case Study 2julissaBelum ada peringkat
- INSPIRIUM BR 2Dokumen32 halamanINSPIRIUM BR 2Sanja PaunicBelum ada peringkat
- Campbell, James - CV - 25 Feb 2016Dokumen42 halamanCampbell, James - CV - 25 Feb 2016meenakshi.r.agrawalBelum ada peringkat
- Hematología - Williams (Tomo 1)Dokumen1.036 halamanHematología - Williams (Tomo 1)LIliana100% (3)
- PedsQL Scoring PDFDokumen146 halamanPedsQL Scoring PDFRam Pokharel100% (1)
- Use of Umbrella Graft For Nasal Tip ProjectionDokumen4 halamanUse of Umbrella Graft For Nasal Tip ProjectionbsBanBelum ada peringkat
- Hypnosis For Children Undergoing Dental TreatmentDokumen22 halamanHypnosis For Children Undergoing Dental TreatmentPuteri MentariBelum ada peringkat
- Fungal RhinosinusitisDokumen5 halamanFungal RhinosinusitisigorBelum ada peringkat
- List of Private Hospitals and Diagnostic Centers Approved by INSADokumen16 halamanList of Private Hospitals and Diagnostic Centers Approved by INSAvijay sainiBelum ada peringkat
- 11 Congenital Pouch Colon: Devendra K. Gupta and Shilpa SharmaDokumen11 halaman11 Congenital Pouch Colon: Devendra K. Gupta and Shilpa SharmaRudi haris munandarBelum ada peringkat
- DR Suman Thapa - Challenges of Glaucome Care in The HimalayasDokumen54 halamanDR Suman Thapa - Challenges of Glaucome Care in The HimalayasAn Da100% (1)
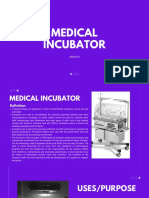
- Medical Incubator 1Dokumen6 halamanMedical Incubator 1Yan YanBelum ada peringkat
- NeuropsychiatryDokumen5 halamanNeuropsychiatryNicole TangcoBelum ada peringkat
- Acute and Chronic Gastritis Due To Helicobacter PyloriDokumen8 halamanAcute and Chronic Gastritis Due To Helicobacter PyloriCarla HolandBelum ada peringkat
- Ataxia in ChildrenDokumen9 halamanAtaxia in ChildrenMuhammad Irvan AvandiBelum ada peringkat
- Peds Practice TestDokumen22 halamanPeds Practice TestJoslyn Gross75% (4)
- Child Birth and The Natural BirthDokumen10 halamanChild Birth and The Natural BirthMohan Perera100% (17)
- 8 Films Medical Students Should SeeDokumen3 halaman8 Films Medical Students Should SeehrfarahanchiBelum ada peringkat
- Systemic Vasculitis: Poonam Sharma, Mbbs Sanjeev Sharma, MD Richard Baltaro, MD and John Hurley, MDDokumen10 halamanSystemic Vasculitis: Poonam Sharma, Mbbs Sanjeev Sharma, MD Richard Baltaro, MD and John Hurley, MDHernan Del CarpioBelum ada peringkat
- Chapter 7: Ear, Nose, and Throat: Published: July 2016Dokumen3 halamanChapter 7: Ear, Nose, and Throat: Published: July 2016ab_ghaffar_latiffi9337Belum ada peringkat
- Implant Occlusion Articles AbstractDokumen4 halamanImplant Occlusion Articles AbstractMrunal DoiphodeBelum ada peringkat
- Powerpoint PresentationDokumen34 halamanPowerpoint Presentation88AKK100% (2)
- Bone Tumor - Dr. Andri R. Winoto, SpOT (K)Dokumen19 halamanBone Tumor - Dr. Andri R. Winoto, SpOT (K)Aramanda DianBelum ada peringkat
- Skeletal Anchorage in OrthodonticsDokumen8 halamanSkeletal Anchorage in OrthodonticsNingombam Robinson SinghBelum ada peringkat
- Best Docs - Aug 09Dokumen18 halamanBest Docs - Aug 09AY Magazine100% (2)
- REDCOP Updates (Reg.v)Dokumen36 halamanREDCOP Updates (Reg.v)DaNiel AUreusBelum ada peringkat
- Pediatric RehabilitationDokumen124 halamanPediatric RehabilitationNalin Kumar100% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (170)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Dari EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Belum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDari EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 4 dari 5 bintang4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDari EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisPenilaian: 5 dari 5 bintang5/5 (8)
- To Explain the World: The Discovery of Modern ScienceDari EverandTo Explain the World: The Discovery of Modern SciencePenilaian: 3.5 dari 5 bintang3.5/5 (51)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDari EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Marshmallow Test: Mastering Self-ControlDari EverandThe Marshmallow Test: Mastering Self-ControlPenilaian: 4.5 dari 5 bintang4.5/5 (59)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDari EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryPenilaian: 4 dari 5 bintang4/5 (45)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDari EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifePenilaian: 4.5 dari 5 bintang4.5/5 (253)