Anda mungkin juga menyukai
- Cyclone Ma HasenDokumen1 halamanCyclone Ma Hasenmarkleongoldber3215Belum ada peringkat
- AVAC AIDS Tipping PointDokumen1 halamanAVAC AIDS Tipping PointmurphmanBelum ada peringkat
- ClimasphereDokumen1 halamanClimaspheremarkleongoldber3215Belum ada peringkat
- 1.1 Million: Philippines: Typhoon Haiyan - Humanitarian SnapshotDokumen1 halaman1.1 Million: Philippines: Typhoon Haiyan - Humanitarian Snapshotmarkleongoldber3215Belum ada peringkat
- Syria Numbers and Locations of Refugees and IDPsDokumen1 halamanSyria Numbers and Locations of Refugees and IDPsmarkleongoldber3215Belum ada peringkat
- TB in South African MinesDokumen2 halamanTB in South African Minesmarkleongoldber3215Belum ada peringkat
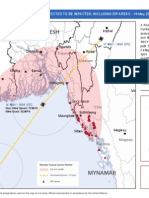
- Cyclone Ma HasenDokumen1 halamanCyclone Ma Hasenmarkleongoldber3215Belum ada peringkat
- Eastern Africa Floods Update 17 May 2013Dokumen1 halamanEastern Africa Floods Update 17 May 2013markleongoldber3215Belum ada peringkat
- Syria DisplacementlRefugees 2013apr05 HIU U770Dokumen1 halamanSyria DisplacementlRefugees 2013apr05 HIU U770markleongoldber3215Belum ada peringkat
- Rotary Info Graphic FINALDokumen2 halamanRotary Info Graphic FINALmarkleongoldber3215Belum ada peringkat
- Hurricane - Sandy 26 October 2012petitDokumen1 halamanHurricane - Sandy 26 October 2012petitmarkleongoldber3215Belum ada peringkat
- RMMS September MapDokumen1 halamanRMMS September Mapmarkleongoldber3215Belum ada peringkat
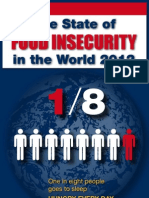
- FAO Infographic SOFI 2012 enDokumen1 halamanFAO Infographic SOFI 2012 enmarkleongoldber3215Belum ada peringkat
- Unhcr Pop of ConcernDokumen2 halamanUnhcr Pop of Concernmarkleongoldber3215Belum ada peringkat
- Ocha FundingDokumen2 halamanOcha Fundingmarkleongoldber3215Belum ada peringkat
- Worldwide HumanitarianAidWorkers 2012aug15 HIU U618Dokumen1 halamanWorldwide HumanitarianAidWorkers 2012aug15 HIU U618markleongoldber3215Belum ada peringkat
- Lebanon RefugeesDokumen1 halamanLebanon Refugeesmarkleongoldber3215Belum ada peringkat
- PakfloodsDokumen1 halamanPakfloodsmarkleongoldber3215Belum ada peringkat
- Saving at BirthDokumen1 halamanSaving at Birthmarkleongoldber3215Belum ada peringkat
- Map of The DayDokumen1 halamanMap of The Daymarkleongoldber3215Belum ada peringkat
- UN Polling Data1Dokumen8 halamanUN Polling Data1markleongoldber3215Belum ada peringkat
- Fall 2011 UN Polling MemoDokumen9 halamanFall 2011 UN Polling Memomarkleongoldber3215Belum ada peringkat
- Ivac-2011 Pneumonia Progress ReportDokumen7 halamanIvac-2011 Pneumonia Progress Reportmarkleongoldber3215Belum ada peringkat
- Speaker Series InvitationDokumen1 halamanSpeaker Series Invitationmarkleongoldber3215Belum ada peringkat
- Map 1293Dokumen2 halamanMap 1293markleongoldber3215Belum ada peringkat
- Somalia MapDokumen2 halamanSomalia Mapmarkleongoldber3215Belum ada peringkat
- Famine MapDokumen1 halamanFamine Mapmarkleongoldber3215Belum ada peringkat
- MogadishuDokumen1 halamanMogadishumarkleongoldber3215Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Chemical WarfareDokumen18 halamanChemical WarfareUnited States Militia100% (2)
- Nerve Agents: A Concise GuideDokumen66 halamanNerve Agents: A Concise GuideAlen SušićBelum ada peringkat
- Integrated Binary Production Facility, Pine Bluff, ArkansasDokumen95 halamanIntegrated Binary Production Facility, Pine Bluff, Arkansasscott_murphey100% (1)
- DHS Terrorism Risk Assessments July 2016 - Part1Dokumen10 halamanDHS Terrorism Risk Assessments July 2016 - Part1caner dereliBelum ada peringkat
- Datasheet CBRN-CAP-1-Canister HS 6574A 0913Dokumen2 halamanDatasheet CBRN-CAP-1-Canister HS 6574A 0913nidhinBelum ada peringkat
- CI Garments - GuideDokumen40 halamanCI Garments - GuideJOSE IGNACIO CEBALLOS RESTREPOBelum ada peringkat
- Chemical and Biological Weapons: DR Carlo KoppDokumen3 halamanChemical and Biological Weapons: DR Carlo KoppYacine KhlilBelum ada peringkat
- Tabun Nerve AgentDokumen4 halamanTabun Nerve AgentPacko Lopez100% (1)
- DHS 103-06 DeconEquip DraftReport 3-19-07Dokumen554 halamanDHS 103-06 DeconEquip DraftReport 3-19-07604joe100% (3)
- Nerve AgentsDokumen24 halamanNerve AgentsIvan JerkovićBelum ada peringkat
- Weapons of Mass DestructionDokumen41 halamanWeapons of Mass DestructionRexchel Nicole P. AlvarezBelum ada peringkat
- Bhopal Original ArticleDokumen7 halamanBhopal Original ArticlespsarathyBelum ada peringkat
- Classification of Poisons: Types, Effects, and ManagementDokumen73 halamanClassification of Poisons: Types, Effects, and ManagementpikachuBelum ada peringkat
- Sarin-Nerve AgentDokumen69 halamanSarin-Nerve AgentAlen Sušić100% (1)
- Military Toxicology Crash Course IntroductionDokumen97 halamanMilitary Toxicology Crash Course IntroductionvrtzioBelum ada peringkat
- A Review of Chemical Warfare Agent (CWA) Detector TechnologiesDokumen109 halamanA Review of Chemical Warfare Agent (CWA) Detector TechnologiesRoberto MichelenaBelum ada peringkat
- CBRN Threat PDFDokumen6 halamanCBRN Threat PDFbta45 Tebet100% (1)
- Unit 3 (STS)Dokumen31 halamanUnit 3 (STS)Angilyn LumabasBelum ada peringkat
- Acetylcholinesterase Inhibitors As Alzheimer Therapy From Nerve Toxins To NeuroprotectionDokumen24 halamanAcetylcholinesterase Inhibitors As Alzheimer Therapy From Nerve Toxins To NeuroprotectionLucasBritoBelum ada peringkat
- Evers SafetyBook V3Dokumen160 halamanEvers SafetyBook V3Gudruman EdisonBelum ada peringkat
- Bota HazmatDokumen2 halamanBota HazmatGuadalupe LechugaBelum ada peringkat
- Nerve Gas: America's Fifteen Year Struggle For Modern Chemical WeaponsDokumen3 halamanNerve Gas: America's Fifteen Year Struggle For Modern Chemical WeaponsReid Kirby100% (1)
- TabunDokumen24 halamanTabunMiftakul SururiBelum ada peringkat
- Presentation in StsDokumen70 halamanPresentation in StsJohn Abe NasayaoBelum ada peringkat
- Corpsman Exam Cheat Sheet! SSIC Codes: Deficiency CausesDokumen6 halamanCorpsman Exam Cheat Sheet! SSIC Codes: Deficiency CausesLueshen WellingtonBelum ada peringkat
- USMC: Lessons Learned From The Iraq-Iran War (Appendix B)Dokumen5 halamanUSMC: Lessons Learned From The Iraq-Iran War (Appendix B)cartalucciBelum ada peringkat
- Nerve AgentsDokumen4 halamanNerve AgentsMaya OlinBelum ada peringkat