Mevalonic Acid & Cholesterol
Diunggah oleh
bram_elibraryJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Mevalonic Acid & Cholesterol
Diunggah oleh
bram_elibraryHak Cipta:
Format Tersedia
Urinary excretion of mevalonic acid as an indicator of
cholesterol synthesis
Bernhard Lindenthal,* Abraham Simatupang,* Maria Teresa Dotti,?Antonio Federico,t
Dieter Liitjohann,* and Klaus von Bergma".*
Department of Clinical Pharmacology,* University of Bonn, Sigmund-FreudStrasse25, 53 105 Bonn,
Germany, and Istituto di Scienze Neurologiche,+Universita di Siena, Siena, Italy
Abstract Urinary excretion of mevalonic acid was investi- this diurnal variation in serum concentrations of
gated as an indicator of cholesterol synthesis. In normoli- mevalonic acid, a significant correlation between
pemic volunteers, excretion of mevalonic acid averaged 3.51
f 0.59 (SD) pg,/kg x day'; (n = 24) and was not different from mevalonic acid in fasting serum and total cholesterol
patients with hypercholesterolemia(3.30 f 0.92 pdkg x day'; synthesis measured by the fecal balance method has
n = 24). In patients with cerebrotendineous xanthomatosis, been observed under metabolic ward conditions (3).
the excretion was significantly higher (8.55 f 1.92 pg/kg x Under outpatient conditions, however, Popjak et al. (4)
Downloaded from www.jlr.org by on May 24, 2009
day'; n = 6, P < 0.001) but comparable to volunteers treated and Parker et al. (2) noted a large variation on different
with cholestyramine (6.69 f 2.6 pglkg x day'; n = 5). A
significant correlation was found between 24-h excretion of days in the serum concentrations of individual subjects.
mevalonic acid and cholesterol synthesis (r = 0.835; n = 35; P For this reason, it may be difficult to estimate cholesterol
< 0.001). The coefficient of variation of excretion of mevalo- synthesis rates in outpatients by measuring serum con-
nic acid during 3 consecutive days was small (9.8%;n = 7). centrations of mevalonic acid. As mevalonic acid from
However, urinary output of mevalonic acid was significantly serum is excreted rapidly into urine, a 24h urinary
higher during the night (164 f 14 pg/12-h) than during the
day (129 f 9 ~ g A 2 - hn; = 11; P < 0.05). In patients treated excretion of mevalonic acid provides a measurement of
with simvastatin (40 mg/day) for 6 weeks, the ratio of mevalo- the integrated serum concentrations of mevalonic acid
nic acid to creatinine in a morning urine sample decreased (5, 6). Therefore, daily excretion of mevalonic acid
significantly compared to pretreatment values (1 10 f 25 pg/g might be a better indicator of total cholesterol synthesis
vs. 66 f 25 pug;P < 0.001). Furthermore, the ratio of mevalo- (7). Indeed, it has been demonstrated that inhibition of
nic acid to creatinine in a morning urine sample correlated
with the ratio from the 24h collection period (r = 0.714; n = cholesterol synthesis by HMG-CoA reductase inhibitors
34; P < 0.001). The results indicate that the analysis of uri- reduces urinary outputs of mevalonic acid (8, 9),
nary mevalonic acid, either in 24h collection or in a single whereas stimulation of bile acid synthesis by administra-
morning sample, is an attractive method for evaluation of tion of a bile acid binding resin has the opposite effect
long and very short term changes of the rates of cholesterol
synthesis.-lindent, B., A. Simatupang, M. T. Dotti, A. (299).
Federico, D. Liitjohann, and K. von Bergmann. Urinary In the present study we selected healthy normoli-
excretion of mevalonic acid as an indicator of cholesterol pemic volunteers and patients with primary hyper-
synthesis.J.Lipid Res. 1996. 37: 2193-2201. cholesterolemia and tested the hypothesis that the 24h
urinary excretion of mevalonic acid reflects cholesterol
Supplementary key words simvastatin lovastatin pravastatin synthesis measured by fecal balance. Twenty-four-hour
cholestyramine hypercholesterolemia diurnal variation of choles-
terol synthesis fecal balance stable isotope urinary excretion rates of mevalonic acid were also
measured in patients with the rare inherited disease of
cerebrotendinous xanthomatosis (CTX) who are known
The conversion of 3~-hydroxy-3~-methylglutaryl co- to have elevated cholesterol synthesis rates (10).Further-
enzyme A (HMGCoA) into mevalonic acid regulated by
HMGCoA reductase is the rate-limiting step in choles-
terol biosynthesis (1). In the metabolic steady state, the
serum concentrations of mevalonic acid reflect the ac- Abbreviations:HMG-CoA, 3~hydroxy-3f!-methylglutaaryl
coenzyme
tivity of hepatic HMGCoA reductase, including its peak A; CTX, cerebrotendinous xanthomatosis; GLC/MS, gas-liquid
chromatography-mass spectrometry; SIM,selected ion monitoring;
concentrations at night and low concentrations during HDL, high density lipoprotein; LDL, low density lipoprotein.
the day that may vary 2- to 5-fold over 24 h (2). Despite 'To whom correspondenceshould be addressed.
Journal of Lipid Research Volume 37,1996 2193
more, we investigated whether the diurnal rhythm of treated with a low dose of 10 mg q.d. or 10 mg b.i.d., 19
serum mevalonic acid can also be detected in urinary with a medium dose (20 mg q.d. or 20 mg b.i.d,), and 9
output, when the sampling time is divided into day and with a high dose (40 mg q.d. or 40 mg b.i.d.) of simvas-
night time. Finally, we tested the hypothesis that the tatin or lovastatin, respectively. Patients received the
ratio of mevalonic acid to creatinine in a single fasting treatment for at least 6 weeks. The results were com-
urine sample could be used to indicate changes in pared to 18 patients without lipid-lowering drugs,
cholesterol synthesis. matched for age, sex, and body weight. All subjects and
patients gave informed consent and all the studies were
approved by the local ethical committee.
PATIENTS AND METHODS
Measurement of mevalonic acid
Subjects
Mevalonic acid in urine was determined by method 3
Twenty-four normolipemic male volunteers (con- previously reported (11). Briefly, 60.2 ng of
trols) aged 22 to 32 years, 24 patients with primary [2H3]mevalonicacid (MSD Isotopes, Montreal, Canada)
hypercholesterolemia (15 men and 9 women) aged 26 was added as internal standard to 400 pl urine. After
to 68 years, and 6 patients with CTX (3 men and 3 extraction, purification, and derivatizationwith methyl-
women) aged 29 to 45 years participated in the study. tertiary-butyldimethylsilyl-trifluoracetamide,the con-
Diabetes, renal/liver disease, or thyroid dysfunction centration of mevalonic acid was analyzed by gas-liquid
were excluded by history and laboratory means, and chromatography/mass spectrometry (GLC/MS) on a
none of the volunteers or patients were treated with Hewlett-Packard(HP) GLC 5890 combined with an HP
drugs known to influence cholesterol metabolism. In 5970 quadropole type MS. Selected ion monitoring
Downloaded from www.jlr.org by on May 24, 2009
patients with CTX, chenodeoxycholic acid administra- (SIM) was performed by cycling the quadropole mass
tion was stopped 4 weeks before the study. The clinical filter between m/z values at a rate of 5.2 cycles per
profile and lipoprotein concentrations of the different second. In the SIM mode, the ion m/z 317 (base peak)
groups of subjects are summarized in Table 1. was scanned for authentic mevalonic acid and the ion
m/z 320 for [*Hs]mevalonicacid. Creatinine in urine was
Study design
measured by a standard laboratory procedure.
Seven different kinds of studies were performed. 1)
Measurement of 24h urinary mevalonic acid was ob- Cholesterol synthesis
tained in all normolipemic subjects, patients with hyper-
cholesterolemia, and CTX. 2) In 12 of the volunteers Fecal samples for sterol balance measurements were
and in 23 of the patients with hypercholesterolemia, collected and analyzed as described elsewhere (12). For
fecal balance measurements for total cholesterol synthe- this purpose, subjects received sitostanol (30 mg t.i.d.)
sis were carried out during the week of the 24-h urine for 7 days as fecal flow and recovery marker and stools
collections. 3) Seven subjects collected urine for 3 con- were collected on days 5, 6, and 7 for GLC analysis of
secutive days under metabolic ward conditions and neutral and acidic sterols. Daily cholesterol intakes were
again 4 weeks later for 3 consecutive days as outpatients. calculated from 7day food records using a computer
4) In 11 volunteers the 24h urinary collections were program for food composition (13).The rate of choles-
divided into two 12-h periods, the first from 7.00 terol synthesis was then estimated by subtracting the
AM-7.00PM (day)and the second one from 7.00 PM-7.00 daily intake of cholesterol from total daily fecal sterol
AM (night).5) Seven volunteers collected urine for 24-h
excretion (12).
before and after 6 weeks of administration of pravastatin Lipid and lipoprotein analysis
(20 mg at bedtime), and 5 volunteers collected urine
before and during the last day of cholestyramine treat- Blood was drawn for serum lipid and lipoprotein
ment (4 g b.i.d. for 2 weeks). 6) In 21 of the volunteers analysis in the morning after an overnight fast. Total
and in 13of the patients with hypercholesterolemia,an cholesterol and triglycerides in serum were measured
additional urine fasting specimen was collected after the by enzymatic methods (Boehringer, Mannheim, Ger-
completion of the 24-h urine collection period. 7) many). High density lipoprotein (HDL) cholesterol was
Mevalonic acid concentrations were measured in a also determined enzymatically in the supernatant after
morning urine specimen in 12 patients with hyper- precipitation of apolipoprotein B-containing lipoprote-
cholesterolemia before and after 6 weeks of treatment ins with heparin-manganese (Boehringer, Mannheim,
with simvastatin (40 mg/day). A morning urine sample Germany). Low density lipoprotein (LDL) cholesterol
was also obtained in patients treated with different doses was calculated by the method of Friedewald, Levy,and
of an HMGCoA reductase inhibitor. Six patients were Fredrickson (14).
2194 Journal of Lipid Research Volume 37,1996
TABLE 1. Clinical data and lipoprotein concentrationsin normolipemicvolunteers, patients with
hvnercholesterolemia.and Patients with cerebrotendinousxanthomatosis(CTX)
Hypercholesterolemic CTX
Controls Patients Patients
Variable n=24 n = 24 n=6
Age (yr) 27f3 50 f 12O 39 f 6'
(21-32) (26-68) (29-45)
Body weight (kg) 83 f 14 76 f 14" 54 f 7b
(62-122) (50-98) (46-65)
BMI (kg/mP) 25 f 4 25 f 3 20 f 2'
(20-40) (22-30) (17-23)
Cholesterol (mddl) 182 It 21 314 f 5Q 143 f 164.
(147-229) (237-452) (120-160)
LDLcholesterol (mg/dl) 109 f 19 243 f 56n nd
(75-146) (160-396)
HDL-cholesterol (mg/dl) 55 f 12 44flOIl nd
(34-74) (29-62)
Triglyceride (mg/dl) 83 f 18 133 f 38' nd
(46-108) (65-212)
Cholestanol (mg/dl) nd nd 2.4 f 1.B
(1.1-4.4)
Values are given as means f SD; range in parentheses;n, number of subjects; nd, not done.
"Significantlydifferent from controls, P < 0.05.
'Significantly different from controls and patients with hypercholesterolemia,P < 0.05.
'Measured by gas-liquid chromatography.
Downloaded from www.jlr.org by on May 24, 2009
Analysis of cholestanol and cholesterol by gas-liquid Statistical analysis
chromatography The results are expressed as mean f standard devia-
Analysis of cholesterol and cholestanol was per- tion (mean k SD) to show variations in a group or as
formed as described previously (15). Briefly, to 100 pl standard error of the mean (SEM) to compare different
of serum 50 pg of 5a-cholestane (ServaFeinbiochemica, groups. Differences between paired or unpaired results
Heidelberg, Germany) was added as internal standard. were calculated using the Student's t-test and considered
After alkaline hydrolysis and extraction with n-hexane, significant at a level of P < 0.05. The correlationbetween
cholesterol and cholestanol were derivatized to their parameters was tested by Pearson's correlation coeffi-
trimethylsilylethers and quantified by GLC. cient. Coefficients of variation (CV) were calculated as
SD/mean x 100%. All calculations were done with the
statistical software of SPSS/Windows (SPSS Inc.).
Calculation of the amount of mevalonic acid
excreted in urine and not used for cholesterol
synthesis RESULTS
As 6 moles of mevalonic acid are incorporated into
cholesterol (16) it was possible from the present results Twenty-fourhoururinary excretion of mevalonic
to calculate the percentage of mevalonic acid excreted acid in different groups of subjects
in urine and not used for cholesterol synthesis by the Twenty-four-hour urinary excretions of mevalonic
following equations: acid in normolipemic volunteers, in patients with hyper-
cholesterolemia,and patients with CTX are summarized
in Table 2. In the control subjects, excretion of mevalo-
Mevalonic acid((=)(mol/day) =
nic acid averaged 288 pg/day, and was slightly (but
cholesterol synthesis (mol/day) x 6 Eq. 1) significantly)higher (14%) than in patients with hyper-
cholesterolemia (249 pg/day; P < 0.05). As the weights
Mevalonic acid (U) (%) = [mevalonic acid of the volunteers were also slightly (but significantly)
(U) (mol/day) / mevalonic acid higher than those of the hypercholesterolemicpatients,
(C) (mol/day)] x 100% Eq. 2 ) no significant difference could be detected after correc-
tion for body weight or when expressed as ratio to
where (C) is the amount used for cholesterol synthesis creatinine (Table 2). These results demonstrate that
and (U) the amount excreted in urine. there were no differences in the rates excretion of
Lindathal et al. Urinary mevalonic acid as indicator of cholesterol synthesis 2195
TABLE 2. Excretion of mevalonic acid in 24h urine of normolipemicvolunteers (controls),patients with
hypercholesterolemia,and patients with cerebrotendmousxanthomatosis (CTX)
Mevalonic Mevalonic Acid Mevalonic Acid
Subjecu Acid per Body Weight per Creatinine
Why Wkx day.' Pdg day'
Volunteers (n = 24) 288 f 54 3.51 f 0.59 142 It 22
(167-428) (2.57-4.43) (93- 177)
Hypercholesterolemic
patients (n = 24) 249 f 82" 3.30 f 0.92 158 f 52
(89-398) ( 1.53-5.04) (89-266)
CTX patients (n = 6) 467 f 1416 8.55 f 1.9Z6 424 f 376
(312-678) (5.67-10.43) (350-449)
Values are given as means f SD; range in parentheses.
"Significantlydifferent from volunteers,P < 0.05.
bSignificantly different from volunteers and hypercholesterolemic patients, P < 0.001.
mevalonic acid between normolipemic volunteers and muday) and is independent of hypercholesterolemia
patients with hypercholesterolemia. Although dietary and gender.
cholesterol intake was significantly higher in volunteers
Reproducibility of daily excretion of mevalonic acid
(291 k 70 muday) than in patients with hypercholeste-
rolemia (179 k 89 muday; P < 0.05) this difference did To investigate the reproducibility of the daily excre-
not affect mevalonic acid excretion. In contrast, the tion of mevalonic acid, the day to day variation in
Downloaded from www.jlr.org by on May 24, 2009
rates of daily urinary excretion in patients with CTX urinary excretion of mevalonic acid was evaluated in 7
were on the average 1.6-and 1.9-fold higher than those volunteers over 3 consecutive days, first under metabo-
in volunteers and in hypercholesterolemia patients, and ,lit ward conditions and second 4 weeks later as outpa-
even 2.5-fold higher when expressed to body weight m tients. The results of this study are given in Table 3. The
as ratio to creatinine (P< 0.001). coefficient of variation of excretion of mevalonic acid
was low and remained the same whether collected under
Correlationbetween urinary excretion of mevalonic metabolic ward conditions (range: 3.5% to 14.3%, mean
acid and cholesterol synthesis 9.2%) or as outpatients (range: 2.2% to 16.2%; mean
Twenty-four-hoururinary excretion of mevalonic acid 9.8%). Although there were some differences in total
was compared to the rate of total cholesterol synthesis daily output from subject to subject, the overall excre-
in 12 normolipemic volunteers and 23 patients with tion rates were not different between metabolic ward or
hypercholesterolemia. Total cholesterol synthesis was outpatient conditions (285 pg/day vs. 287 pdday).
significantly correlated to excretion of mevalonic acid (T
= 0.835; P < 0.001; Fig. 1). There was no difference in
the slope of the line between normolipemic volunteers
(y = 0 . 1 8 ~+ 80; r = 0.655; P < 0.02) and patients with
hypercholesterolemia (y = 0 . 2 1 ~ + 19; r = 0.897; P <
0.001). No relation between mevalonic acid excretion
and dietary intake of cholesterol was seen, but excretion
of mevalonic acid was also related to body weight ( T =
0.607; P < 0.001; n = 48) (data not shown). From the
combined measurements of total cholesterol synthesis
and 24-h urinary excretion of mevalonic acid, the per-
centage of mevalonic acid not used for cholesterol syn-
thesis and that spilled over into urine was calculated.
Normolipemic volunteers excreted a calculated average
of 0.01 1f 0.002% (SD), that was identical to that in male " 8
(0.011 f 0.002%), and female patients with hyper- 0 400 800 1200 1600 2000
cholesterolemia (0.010 f0.001%). The data indicate that Cholesterol Synthesis (mg/day)
the percentage of mevalonic acid that escapes choles-
Fig. 1. Comparison of cholesterol synthesis measured by fecal bal-
terol synthesis is extremely constant over the whole ance and 24h urinary excretionof mevalonic acid in 12 normolipemic
range of total cholesterol synthesis (560 m u d a y to 1790 healthy volunteers and 23 patients with hypercholesterolemia.
2196 Journal of Lipid Research Volume 37, 1996
TABLE3. Excretion of mevalonic acid in 24h urine from seven 34; Fig. 3). Furthermore, the ratio of mevalonic acid to
normolipemic volunteers (controls)on 3 consecutive days under creatinine in the morning urine specimen also corre-
metabolic ward and outpatient conditions
lated to the daily excretion of mevalonic acid ( r = 0.541;
Mevalonic Acid
P < 0.001). Thus, even the ratio of mevalonic acid to
Volunteer Metabolic Ward Outpatient
creatinine in a singleurine sample can give an indication
1 254 f 36 Why 312 f 36 of the cholesterol synthesis in individual subjects.
(14.3) (11.5)
254 f 40
Effect of simvastatin and lovastah on mevalonic
2 286 f 39
(13.5) (16.2) acid concentrations in a morning urine sample
3 272 f 9.5 321 f 31 In order to test further this hypothesis that mevalonic
(3.5) (4.8) acid in a single urine specimen is valid for showing
4 253 + 24 263 f 20
changes in cholesterol synthesis, we compared the ratio
(9.2) (5.7)
5 283 f 14 348 f 21 of mevalonic acid to creatinine in the morning urine
(5.0) (2.2) specimens in 12 hypercholesterolemic patients before
6 326 f 42 356 f 17 and after 6 weeks of treatment with simvastatin (40
(12.8) (15.9) muday). The ratio of mevalonic acid to creatinine was
7 321 f 19 223 f 27
(5.8) (12.0) lowered in all subjects, on the average by 40%, from 110
Mean f SEM 285 f 11 287 f 19 f 25 lg/g to 66 f 25 pg/g (P < 0.001). The individual
results are shown in Fig. 4. In addition, the ratio of
Values are given as mean f SD; coefficient of variation (SD/mean
x 100[%]) in parentheses. mevalonic acid to creatinine was measured in patients
treated with different doses of simvastatin or lovastatin
and compared to matched patients with hyper-
Downloaded from www.jlr.org by on May 24, 2009
Diurnal variation in excretion of mevalonic acid cholesterolemia without lipid lowering therapy (Table
4). A significantly lower ratio of mevalonic acid to
Dividing 24h urine collections in two periods of time,
creatinine was seen with all three different doses com-
a significantly higher output of mevalonic acid was seen
pared to no lipid lowering therapy (P< 0.01). However,
during the night than during the day (P < 0.05; Fig. 2).
no further significant reduction was seen between the
However, in 3 out of 11 volunteers, the excretion during
low, medium or high dose of the two HMG-CoA reduc-
the day was slightly higher than during the night (4%,
tase inhibitors.
18%,and 20%). In the 8 subjects where the output was
higher during the night than during the day, the excre-
tion of mevalonic acid was 46% higher at night (range
DISCUSSION
6% to 122%).
Effect of pravastatin and cholestyramine on Measuring cholesterol synthesis provides us with im-
excretion of mevalonic acid portant information on cholesterol homeostasis under
As expected, pravastatin decreased 24h excretion of various physiological conditions, disease states, and
mevalonic acid in all 7 volunteers, on the average by 38%
from 293 f 65 mg/day to 196 f 52 mg/day (P < 0.02).
The bile acid binding resin, cholestyramine, increased
urinary output on the average from 305 f 97 mg/day to
487 f 137 mg/day (+60%;P < 0.02; n = 5).
200 -
p < 0.05 /
Excretion of mevalonic acid during 24 h and
concentrationsmeasured in a morning urine sample
To study the possibility that measurement of mevalo-
nic acid in a spontaneous fasting urine sample collected 100 -
in the morning is suitable as an indicator of changes in
cholesterol synthesis rates, we compared the results with
those from the 24h collections. The results of 24-h
urinary excretion of mevalonic acid in volunteers and
"
patients with hypercholesterolemia compared to those Day Night
from a single fasting urine sample from the same subject
showed a significant positive correlation when ex- Fig. 2. Urinary excretion of mevalonic acid during the day (7.00
AM-7.00PM) and the night (7.00 PM-7.00AM) in 11 normolipemic
pressed as ratio to creatinine ( r = 0.714; P < 0.001; n = volunteers.
Lindathal et al. Urinary mevalonic acid as indicator of chdesterol synthesis 2197
MVA/Crea. (in a morning urine sample) also revealed no difference between normolipemic con-
trols and patients with hypercholesterolemia (14.2
mg/kg x day' vs. 14.3 mg/kg x day'). Previous studies
have also indicated that patients with heterozygous fa-
milial hypercholesterolemia do not or only slightlydiffer
/ -
in their total cholesterol synthesis from controls (17), or
in their biliary secretion rates of cholesterol and bile
acids (18, 19). Thus, the present results of excretion of
100 mevalonic acid are in accordance with studies per-
formed previously on cholesterol metabolism in pa-
50
tients with hypercholesterolemia (17-19).
" I
Patients with CTX showed a 2.5-fold higher secretion
0 50 100 150 200 250 300 rate of mevalonic acid per body weight compared to
MV#Crea. (In 24-h urine) volunteers and patients with hypercholesterolemia. Pre-
(PleIEl) vious studies using the fecal balance method also
showed a higher total cholesterol synthesis in two pa-
Fig. 3. Comparison of the ratio of mevalonic acid to creatinine in tients with CTX compared to five controls (18.2 mg/kg
urine collected for 24 h and in a morning specimen collected imme-
diately after the 24-h collection period in 34 subjects. x day' vs. 11.1m u k g x day') (lo), but bile alcohols were
not included in the calculation. Whereas fecal balance
is the standard procedure for measuring total choles-
drug treatment. Previous studies have shown that serum terol synthesis (20,21), it is more difficult to perform in
patients with CTX for at least two reasons. First, patients
Downloaded from www.jlr.org by on May 24, 2009
concentrations of mevalonic acid might be useful in
estimating the rate of cholesterol synthesis under meta- with this inherited metabolic disease excrete not only
bolic ward conditions. However, quantification of fecal neutral and acidic sterols but also different bile
mevalonic acid in serum is more difficult than in urine, alcohols; quantification of bile alcohols is more difficult
because of lower concentrations and high serum pro- to perform. Second, bile alcohols are also excreted in
teins. In addition, serum concentrations of mevalonic urine in considerable amounts as glucuronides and
acid show a circadian rhythm and outpatients have large sulfates. In order to calculate the total cholesterol syn-
intraindividual variations, making an evaluation more thesis, bile alcohols from the feces and urine must be
difficult (2,4). Measurements of 24-h urinary excretion added to neutral and acidic fecal sterols. This was not
reflect the integrated serum concentration and could done by Salen and Grundy (10) during their fecal bal-
overcome these pitfalls. Therefore, we focused the pre- ance study. Measuring the excretion of mevalonic acid
sent study on the urinary excretion of mevalonic acid as overcomes this problem. Serum levels of lathosterol also
an indicator of cholesterol metabolism under various correlate with total cholesterol synthesis under various
conditions in humans, using a simple method developed conditions (22) but not all (23). Indeed, Wolthers et al.
in our laboratory (11). (24) found elevated serum concentrations of lathosterol
Twenty-four-hourexcretion of mevalonic acid in
different groups of subjects MVNCroa. wag) (In a morning urine umple)
The results of urinary excretion of mevalonic acid in
normolipemic volunteers and in patients with hyper-
150 - p < 0.001
cholesterolemia obtained during the present study are
consistent with earlier reports by Kopito and Brunnen-
graber (6),Parker et al. (3), and Pappu and Illingworth loo
(9). No significant differences of mevalonic acid excre-
tion could be detected between the two groups when
the results were expressed to body weight or to creat- 50
inine excretion. The 24-h excretion of mevalonic acid
was independent of dietary cholesterol intake. This is in
contrast to previous studies where low and high choles-
0
terol intakes were compared (3), but might be the result Control Shmrrutatin
of the small range of dietary cholesterol intake during
Fig. 4. Ratio of mevalonic acid to creatinine in a morning urine
the present study (only three subjects had a cholesterol sample before and after 6 weeks of treatment with simvastatin (40
intake above 400 muday). Total cholesterol synthesis muday) in 12 patients with hypercholesterolemia.
4198 Journal of Lipid Research Volume 37, 1996
in patients with CTX, another indication of high synthe- synthesis and excretion of mevalonic acid was seen over
sis rates in this disease. Assuming that 0.01% of total a wide range of cholesterol synthesis in both normoli-
cholesterol synthesis is also excreted as mevalonic acid pemic volunteers and patients with hypercholeste-
in urine in patients with CTX, the calculated total syn- rolemia. As total body weight is an important factor in
thesis in our patients would be 34 mg/kg x day'. Com- regulating cholesterol synthesis (25-27), it is obvious
pared to the results of Salen and Grundy (10) almost that excretion of mevalonic acid is also related to body
half of total cholesterol synthesized must have been weight. From the combined measurements of total cho-
converted into bile alcohols. Thus, the higher excretion lesterol synthesis and 24h urinary excretion of mevalo-
of mevalonic acid measured in the six patients with CTX nic acid it was possible to calculate the percentage of
is in line with the considerable amounts of bile alcohols mevalonic acid excreted in urine and not converted to
produced by the patients. The high mevalonic acid cholesterol. The percentage was extremely low but con-
output and total cholesterol synthesis in patients with stant, and independent of age, weight, sex, and choles-
CTX is probably due to the reduced feedback inhibition terol synthesis. It should be mentioned that this calcula-
of cholesterol 7a-hydroxylaseand subsequent inhibition tion does not include the incorporation of mevalonic
of HMGCoA reductase in the liver. As the synthesis of acid into nonsterol isoprenoids (1).
bile acids is regulated by the quantity of these substances
that return to the liver in the enterohepatic circulation, Reproducibility of daily excretion of mevalonic acid
a blockage of bile acid synthesis reduces this quantity
and releases the feedback inhibition. The huge amounts The small intraindividual variations in the daily uri-
of bile alcohols formed by these patients do not down- nary output over 3 consecutive days, measured either
regulate the key enzymes for bile acid and cholesterol under metabolic ward or outpatient conditions, support
synthesis. The mechanism of increased urinary excre- our hypothesis that urinary mevalonic acid is an excel-
Downloaded from www.jlr.org by on May 24, 2009
tion of mevalonic acid in patients with CTX is compara- lent marker for measuring short term changes in cho-
ble to treatment with a bile acid binding resin. During lesterol synthesis. Even minor changes in the rates of
the present study the administration of cholestyramine cholesterol synthesis could be detected by this method.
resulted in excretion rates of mevalonic acid similar to
Diurnal variation in excretion of mevalonic acid
patients with CTX (487 pg/day vs. 467 pg/day).
The diurnal variations in cholesterol synthesis, meas-
Correlation between excretion of mevalonic acid ured either by the activity of the HMGCoA reductase
and cholesterol synthesis
or the serum concentration of mevalonic acid, have not
Results from the present study confirm the close been explained in detail. Parker et al. (3) demonstrated
relationship seen between cholesterol synthesis and that fasting and cholesterol feeding affects the diurnal
mevalonic acid metabolism. Previous investigators com- rhythm. In addition, Pappu and Illingworth (28) noted
pared the plasma concentration of mevalonic acid with similar diurnal variations in patients with homozygous
the results of fecal balance under metabolic ward condi- hypobetalipoproteinemia. Their cholesterol absorption
tions (3).However, Popjak et al. (4) and Parker et al. (2) is negligible (29); thus, mechanisms other than dietary
noted a large variation in the concentration of plasma cholesterol must also play a role in the diurnal variation.
mevalonic acid during outpatient conditions. We, there- The present investigation tested whether the diurnal
fore, in the present study used 24h excretion rates. Daily variation can also be observed in urinary output of
excretion rates may be more reliable for this purpose mevalonic acid. The results confirm previous observa-
because they provide a measure of the integrated serum tions in animals and humans, according to other meth-
concentrations of mevalonic acid (5,6). Although, it has ods that show cholesterol synthesis has a circadian
previously been documented that measuring choles- rhythm (2, 28, 30, 31). It is of interest to note that not
terol synthesis by the fecal balance method is reproduc- every subject exhibited greater excretion rates at night
ible under outpatient conditions (12),it is still necessary than during the day, reported also by other investigators
to use markers for several days to reach steady state fecal using mass isotope distribution analysis (31). Thus, it
excretion and to assess dietary cholesterol intake. It is might be worthwhile to investigate in more detail those
thus an advantage to obtain synthesis rates by a 24-h subjects with a weakened or an inverse diurnal rhythm.
excretion of mevalonic acid. The present results con- The 2-part 24h urine sampling for measurements of
vincingly demonstrate for the first time that 24-h urinary mevalonic acid provides a simple approach for investi-
output of mevalonic acid is highly correlated to rates of gating the mechanism(s) that cause the diurnal peri-
cholesterol synthesis (Fig. 1). As cholesterol synthesis odicity of cholesterol synthesis in humans. In addition,
increases, urinary output of mevalonic acid also be- it can be performed under outpatient conditions and no
comes greater. This relationship between cholesterol blood sampling at night is necessary.
Lindenthal et al. Urinary mevalonic acid as indicator of cholesterol synthesis 3199
TABLE 4. Effect of different doses of simvastatin and lovastatin on the ratio of mevalonic acid to creatinine
in patients with primary hypercholesterolemia in one urine specimen obtained between 8.00 AM and 10.00 AM
Drug n Dose Mevalonic AciWCrearinine
W h Y w g
None 18 169 f 40
Simvastatin 1 x 10
or 6 108 f 1 7 O
Lovastatin 2x10
Simvastatin 1x 2 0
or 19 98 f 7.
Lovastatin 2x20
Simvastatin 1x 4 0
or 9 84 f 1 P
Lovastatin 2x40
Values are given as means f SEM;n, number of patients.
“Significantlydifferent from no treatment, P < 0.01.
Effect of pravastatin and cholestyramine on resulted only in a marginally greater reduction in the
excretion of mevalonic acid
Downloaded from www.jlr.org by on May 24, 2009
ratio that was not significant. Pappu et al. (9, 32) did
The finding of reduced excretion of mevalonic acid identical studies with different doses of lovastatin, but
during treatment with an HMG-CoA reductase inhibitor measured daily output of mevalonic acid. They also
and increased output by administration of cholesty- found the largest decrease in mevalonic acid output
ramine confirms previous results (2, 8, 9, 32). Thus, during the administration of lovastatin in a dose of 10
these measurements can be used to investigate the mg twice daily. The higher doses (20 mg and 40 mg
mechanism of action of lipid-loweringdrugs (33). b.i.d.) did not lead to a further reduction in excretion
of mevalonic acid. The results indicate that measuring
Excretion of mevalonic acid during 24 h and mevalonic acid in a spontaneous urine sample in the
concentrations measured in a morning urine sample morning is a simple and reliable way to measure the
The close relationship between the ratio of mevalonic effects of HMG-CoA reductase inhibitors on changes in
acid to creatinine in 24h urine collections with this ratio cholesterol synthesis. It can also be used in clinical
in a spontaneous urine sample measured in the same studies to control patients’ compliance of drug intake.
subject after an overnight fast and the relationship In conclusion, our simplified GLC/MS method of
between 24h urinary output of mevalonic acid offers measuring urinary excretion of mevalonic acid provides
new opportunities to investigate changes in the rate of important information on cholesterol synthesis and can
cholesterol synthesis during short- and long-term studies. be used under diverse conditions to investigate disor-
ders in cholesterol synthesis.l
Effect of simvastatin and lovastatin on mevalonic
acid concentration measured in a morning urine Excellent technical assistance of Mrs. H. Prange, Mrs. K.
sample Wilmersdorf, and secretary help of Mrs. M. Zerlett are grate-
fully acknowledged. The study was supported by research
The ratio of mevalonic acid to creatinine before and grants from the BMET (01EC9402) and from the Deutsche
during treatment with simvastatin in urine samples col- Forschungsgemeinschaft (BE 1673/1-1). B.L. received a grant
lected in the morning in outpatients with hyper- from the Deutsche Forschungsgemeinschaft; A S . received a
cholesterolemia (Fig. 4) proves that this ratio is an grant from the Deutscher Akademischer Austauschdienst
excellent parameter to evaluate changes in rates of (DAAD)for training in Clinical Pharmacology.
cholesterol synthesis. The magnitude of reduction of Munusrript received 15 April 1996 and in revised form 15July 1996.
this ratio is in line with previous reports of 24-h excre-
tions rates (3, 9, 32) and with the results of pravastatin REFERENCES
during the present study in healthy volunteers (-33%).
Low dose administration of lovastatin and simvastatin 1. Goldstein,J. L., and M. S. Brown. 1990. Regulation of the
mevalonate pathway. Nature. 343: 425-430.
also resulted in a striking decrease in excretion of 2. Parker, T. S., D. J. McNamara, C. Brown, 0.Garrigan, R.
mevalonic acid (-36%) compared to results in patients Kolb, H. Batwin, and E. H. Ahrens, Jr. 1982. Mevalonic
without lipid-loweringdrugs. A 2- or 4-fold higher dose acid in human plasma: relationshipof concentrationand
2200 Journal of Lipid Research Volume 37, 1996
circadian rhythm to cholesterol synthesis rates in man. hypercholesterolemia and combined hyperlipidemia In-
h o c . Natl. Acad. Sci. USA. 7 9 3037-3041. fluence of bezafibrate and fenofibrate. J. Lipd k. 2%
3. Parker, T. S., D. J. McNamara, C. D. Brown, R. Kolb, E. 713-723.
H. Ahrens, Jr., A. W. Alberts,J. Tobert, J. Chen, and P. J. 20. Grundy, S. M., E. H. Ahrens, Jr., and T. A. Miettinen.
De Schepper. 1984. Plasma mevalonate as a measure of 1965. Quantitative isolation and gas-liquid chromatogra-
cholesterol synthesis in man.J Clin. Invest. 74: 795-804. phy analysis of total fecal bile acids.J. Lipid Res. 6:
4. Popjak, G., G. Boehm, T. S. Parker, J. Edmond, P. A. 397-410.
Edwards, and A. M. Fogelman. 1979. Determination of 21. Miettinen, T. A., E. H. Ahrens, Jr., and S. M. Grundy.
mevalonate in blood plasma in man and rat. Mevalonate 1965. Quantitative isolation and gas-liquid chroma-
"tolerance" tests in man.J. Lipid Res. 2 0 716-728. tographic analysis of total dietary and fecal neutral sterols.
5. Kopito, R. R., S. B. Weinstock, L. E. Freed, D. M. Mumy, J. Lipid Res. 6 411-424.
and H. Brunengraber. 1982. Metabolism of plasma 22. Kempen, H. J. M., F. C. Glatz,J. A. Gevers Leuven, H. A.
mevalonate in rats and humans.J. Lipid Res. 23: 577-583. van der Voort, and B. M. Katan. 1988. Serum lathosterol
6. Kopito, R. R., and H. Brunengraber. 1980. (R)-mevalon- concentration is an indicator of whole-body cholesterol
ate excretion in human and rat wines. Proc. Nutl. Acud. synthesis in humans.J Lipid Res. 29: 1149-1 155.
Sci. USA. 77: 5738-5740. 23. Duane, W. C. 1995. Serum lathosterol levels in human
7. Jones, P. J., A. S. Pappu, D. R. Illingworth, and C. A. subjects reflect changes in whole body cholesterol synthe-
Leitch. 1992. Correspondence between plasma mevalonic sis induced by lovastatin but not dietary cholesterol.].
acid levels and deuterium uptake in measuring human Lipid Res. 3 6 343-348.
cholesterol synthesis. Eur.J. Clin. Invest. 22: 609-613. 24. Wolthers, B. G., H. T. Walrecht,J. C. van der Molen, G.
8. Capuzzi, D. M., and W. H. Cevallos. 1984. Inhibition of T. Nagel, J. J. van Doormaal, and P. N. Wijnandts. 1991.
hepatic cholesterol and triglyceride synthesis by guana- Use of determinations of 7-lathosterol (5a-cholest-7en-
benz acetate.J. Cardwvusc. Phamcol. 6 Suppl5 S847-52. 3 k l ) and other cholesterol precursors in serum in the
9. Pappu, A. S., and D. R. Illingworth. 1989. Contrasting study and treatment of disturbances of sterol metabolism,
effects of lovastatin and cholestyramine on lowdensity particularly cerebrotendinous xanthomatosis.J Lipid Res.
lipoprotein cholesterol and 24hour urinary medonate 32: 603-612.
Downloaded from www.jlr.org by on May 24, 2009
excretion in patients with heterozygous familial hyper- 25. Nestel, P. J., H. M. Whyte, and D. W. S. Goodman. 1969.
cholestero1emia.J Lab. Clin. Med. 114 554-562. Distribution and turnover of cholesterol in humans. J.
10. Salen, G., and S. M. Grundy. 1973. The metabolism of Clin. Znuest. 48: 982-99 1.
cholestanol, cholesterol, and bile acids in cerebrotendi- 26. Miettinen, T. A. 1971. Cholesterol production in obesity.
nous xanthomatosis.J Clin. Invest. 52: 2822-2835. Circulation. 44: 842-850.
11. Lindenthal, B., and K. von Bergmann. 1994. Detennina- 27. Grundy, S. M., H. Y.I. Mok, and K. von Bergmann. 1976.
tion of urinary mevalonic acid using isotope dilution Regulation of biliary cholesterol secretion in man. In The
technique. Biol. Mass.Spectrom. 23: 445-450. Liver. Quantitative Aspects of Structure and Function. R.
12. Czubayko, F., B. Beumers, S. Lammsfuss, D. Lutjohann,
Preisig, J. Bircher, and G. Paumgartner, editors. Editio
and K. von Bergmann. 1991. A simplified micro-method Cantor, Aulendorf. 393-403..
for quantification of fecal excretion of neutral and acidic 28. Pappu, A. S., and D. R. Illingworth. 1994. Diurnal vari-
sterols for outpatient studies in humans.J. Lipid Res. 32: ations in the plasma concentrations of mevalonic acid in
1861- 1867.
patients with abetalipoproteinemia.Eu7.J. Clin. Invest. 24:
13. Souci, S. W., W. Fachmann, and H. Kraut. 1990. Compo-
698-702.
sition and Nutrition Tables 1989/ 1990.Wissenschaftliche
29. Illingworth, D. R., W. E. Connor, D. S. Lin, andJ. Diliberti.
Verlagsgesellschaft mbH, Stuttgart, Germany.
1980. Lipid metabolism in abetalipoproteinemia: a study
14. Friedewald, W. T., R. I. Levy, and D. S. Fredrickson. 1972.
of cholesterol absorption and sterol balance in two pa-
Estimation of the concentration of lowdensity lipopro-
tients. Gastroenterology. 78: 68-75.
tein cholesterol in plasma, without use of the preparative
ultracentrifuge. Clin. Chem. 18: 499-502. 30. Jones, P. J., and D. A. Schoeller. 1990. Evidence for
15. Lutjohann, D., I. Bjorkhem, U. F. Beil, and K. von diurnal periodicity in human cholesterolsynthesis.]. Lipid
Bergmann. 1995. Sterol absorption and sterol balance in RES.31: 667-673.
phytosterolemia evaluated by deuterium-labeled sterols: 31. Faix, D., R. Neese, C. Kletke, S. Wolden, M. Coutlangus,
effect of sitostanol treatment.J Lapid Res. 36: 1763-1773. C. H. Shackleton, and M. K. Hellerstein. 1993. Quantifi-
16. Bloch, K. 1965. The biological synthesis of cholesterol. cation of menstrual and diurnal periodicities in rates of
Science. 150: 19-28. cholesterol and fat synthesis in humans. J. Lipid Res. 34:
17. Stacpoole, P. W., K. von Bergmann, L. L. Kilgore, L. A. 2063-2075.
Zech, and W. R. Fisher. 1991. Nutritional regulation of 32. Pappu, A. S., D. R. Illingworth, and S. Bacon. 1989.
cholesterol synthesis and apolipoprotein B kinetics: stud- Reduction in plasma lowdensity lipoprotein cholesterol
ies in patients with familial hypercholesterolemia and and urinary mevalonic acid by lovastatin in pFtients with
normal subjects treated with a high carbohydrate, low fat heterozygous familial hypercholesterolemia. Metabolism.
diet.J. Lipid Res. 32: 1837-1848. 38: 542-549.
18. Tangedahl, T. N., A. F. Hofmann, and B. A. Kottke. 1979. 33. Beil, F. U., A. Schrameyer Wernecke, U. Beisiegel, H.
Biliary lipid secretion in hypercholesterolemia. J. Lipid Greten,J. D. Karkas, R. Liou, A. W. Alberts, H. G. Eckardt,
Res. 2 0 125-133. and A. E. Till. 1990. Lovastatin versus bezafibrate: effi-
19. Leks, O., K. M e y e r - m e r , and K. von Bergmann. 1986. cacy, tolerability, and effect on urinary mevalonate. Car-
B b t y lipid secretion in patients with heterozygous familial d i o l o ~77
. SUppl4 22-32.
Lindathal et al. Urinary mevalonic acid as indicator of cholesterol synthtsip 4901
Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDokumen17 halamanM.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research ScholarDr. M. Prasad Naidu100% (1)
- Hydrocarbons CompleteDokumen70 halamanHydrocarbons CompleteGururaj Vasisth100% (3)
- Oman - Drug - Prices - 06 - 04 - 2013Dokumen488 halamanOman - Drug - Prices - 06 - 04 - 2013Anuj Mairh73% (11)
- Neutriderm Moisturising Lotion Reference (Disodium Lauriminodipropionate Tocopheryl Phosphates Potent New Anti-Inflammatory) PDFDokumen2 halamanNeutriderm Moisturising Lotion Reference (Disodium Lauriminodipropionate Tocopheryl Phosphates Potent New Anti-Inflammatory) PDFBecky BeckumBelum ada peringkat
- Ibudilast: 1873 1873 JP Xvi Infrared Reference SpectraDokumen53 halamanIbudilast: 1873 1873 JP Xvi Infrared Reference SpectraDiego VargasBelum ada peringkat
- Citric Acid Cycle PDFDokumen6 halamanCitric Acid Cycle PDFmanoj_rkl_07Belum ada peringkat
- Dna Molecule Model Exercise No. 3 NAME: Shanica E. Surigao Course and Year: Bsed I - ScienceDokumen8 halamanDna Molecule Model Exercise No. 3 NAME: Shanica E. Surigao Course and Year: Bsed I - ScienceShamaica SurigaoBelum ada peringkat
- Oligosaccharides. Polysaccharides. Terpenes.Dokumen182 halamanOligosaccharides. Polysaccharides. Terpenes.Umar M abubakarBelum ada peringkat
- GENIRICDokumen2 halamanGENIRICŃtǿxBelum ada peringkat
- Antilipidemic DrugsDokumen34 halamanAntilipidemic Drugschelle_morales260% (1)
- ProteinDokumen48 halamanProteinAnggito PrayogaBelum ada peringkat
- Electron Transport Chain NotesDokumen14 halamanElectron Transport Chain NotesseanBelum ada peringkat
- Sơ Đ T NG Quát Chu Trình KrebsDokumen3 halamanSơ Đ T NG Quát Chu Trình KrebsNghĩa VõBelum ada peringkat
- Thiazolopyrimidines: A Retrospective Study of Synthesis, Structure-Activity Relationship and Diverse Pharmacological ActionsDokumen12 halamanThiazolopyrimidines: A Retrospective Study of Synthesis, Structure-Activity Relationship and Diverse Pharmacological ActionsRajat GoyalBelum ada peringkat
- BiochemDokumen41 halamanBiochemIram KhanBelum ada peringkat
- Clearbook Presentation Frontrow InternationalDokumen62 halamanClearbook Presentation Frontrow InternationalLinnel Faye C. Malibiran75% (28)
- Polymer Bulletin: Curing of Epoxy Resins With DicyandiamideDokumen2 halamanPolymer Bulletin: Curing of Epoxy Resins With DicyandiamideyigitilgazBelum ada peringkat
- Half Marathon: SS1105 & SS5604 Foundations of Exercise PhysiologyDokumen21 halamanHalf Marathon: SS1105 & SS5604 Foundations of Exercise PhysiologyDamien TanBelum ada peringkat
- Jurnal Referensi Zat BesiDokumen10 halamanJurnal Referensi Zat BesiChaerul TwentyOneBelum ada peringkat
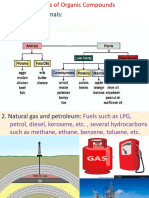
- Sources and Uses of Organic Compounds 3Dokumen13 halamanSources and Uses of Organic Compounds 3Arjun SunarBelum ada peringkat
- Uric Acid Synthesis: By: Michelle S. Sales, RMTDokumen13 halamanUric Acid Synthesis: By: Michelle S. Sales, RMTDayledaniel SorvetoBelum ada peringkat
- Naming AlkenesDokumen22 halamanNaming AlkenesKay AbawagBelum ada peringkat
- Protein FunctionDokumen7 halamanProtein FunctionelixBelum ada peringkat
- Called Saccharides Most Abundant Molecules On Earth Essential Component of All Living OrganismsDokumen32 halamanCalled Saccharides Most Abundant Molecules On Earth Essential Component of All Living OrganismsShyla ManguiatBelum ada peringkat
- Chapter 12 Aldehyde & KetonesDokumen10 halamanChapter 12 Aldehyde & KetonesForzen flamesBelum ada peringkat
- GlycosylationDokumen9 halamanGlycosylationĐỗ Thanh TùngBelum ada peringkat
- Food Packaging Technology: BS-Final Year 18-March-2020Dokumen15 halamanFood Packaging Technology: BS-Final Year 18-March-2020SONIA NABIBelum ada peringkat
- Aldehydes, Ketones and Carboxylic Acids: SolutionDokumen9 halamanAldehydes, Ketones and Carboxylic Acids: SolutionPanchi palBelum ada peringkat
- Product ListDokumen9 halamanProduct ListUsman DarBelum ada peringkat