Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Key Elements of Immunity: SpecificityDokumen9 halamanKey Elements of Immunity: SpecificityParth KulkarniBelum ada peringkat
- Vol.14 No.3 PDFDokumen140 halamanVol.14 No.3 PDFAnn JoseBelum ada peringkat
- Milk Geocities SiteDokumen28 halamanMilk Geocities SiteAmit KasaudhanBelum ada peringkat
- Interesting Q&A in Immunology - Part IIDokumen26 halamanInteresting Q&A in Immunology - Part IIVytheeshwaran Vedagiri90% (10)
- AOM IVIG Comparison Chart 0124 13Dokumen1 halamanAOM IVIG Comparison Chart 0124 13Heba_Al_KhozaeBelum ada peringkat
- September 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityDokumen23 halamanSeptember 26, 2018 by Sagar Aryal: Antigen-Properties, Types and Determinants of AntigenicityEzekiel GantiedBelum ada peringkat
- Medical Microbiology at A Glance EbookDokumen70 halamanMedical Microbiology at A Glance EbookAnkita ShuklaBelum ada peringkat
- Microbiology & Parasitology Module 2 Part 2Dokumen15 halamanMicrobiology & Parasitology Module 2 Part 2BARRERAS Aubrey Eden Faye G.Belum ada peringkat
- Pathogenesis of InfectionDokumen8 halamanPathogenesis of InfectionCardion Rayon Bali UIN MalangBelum ada peringkat
- The Reader Guide To Cure Candida AlbicansDokumen27 halamanThe Reader Guide To Cure Candida AlbicansKyle J. Norton100% (4)
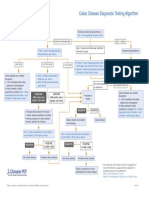
- Celiac Disease Diagnostic Testing AlgorithmDokumen1 halamanCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakBelum ada peringkat
- Immunoglobulins: Submitted byDokumen8 halamanImmunoglobulins: Submitted byNoman AnwarBelum ada peringkat
- Principles of Mucosal Immunology 2020Dokumen615 halamanPrinciples of Mucosal Immunology 2020Trọng PhướcBelum ada peringkat
- Dr. Retno Pudji Rahayu, DRG, M.Kes Depart. Patologi Mulut Dan Maksilofasial FKG UnairDokumen52 halamanDr. Retno Pudji Rahayu, DRG, M.Kes Depart. Patologi Mulut Dan Maksilofasial FKG UnairBima Ewando KabanBelum ada peringkat
- Immune System (Inn & Adapt)Dokumen53 halamanImmune System (Inn & Adapt)Bushra Khan100% (1)
- Presentation FucoidanDokumen42 halamanPresentation FucoidanTaufik Akbar Faried LubisBelum ada peringkat
- Immunological Aspects of Oral DiseasesDokumen35 halamanImmunological Aspects of Oral Diseasesمهدي محمدBelum ada peringkat
- Chapter 3 - Antibody Topic NotesDokumen10 halamanChapter 3 - Antibody Topic NotesAngelica Joy GonzalesBelum ada peringkat
- Immunoglobulins - Structure and Function Definition: Immunoglobulins (Ig)Dokumen9 halamanImmunoglobulins - Structure and Function Definition: Immunoglobulins (Ig)Valdez Francis ZaccheauBelum ada peringkat
- 11 - Psoriasis and Functional Medicine TestingDokumen40 halaman11 - Psoriasis and Functional Medicine TestingAnuj GuptaBelum ada peringkat
- Immunology - Chapter 3 - AntibodiesDokumen56 halamanImmunology - Chapter 3 - AntibodiesMajed IaalyBelum ada peringkat
- SEX and The SKIN - Free E-BookDokumen24 halamanSEX and The SKIN - Free E-Bookbharath_eduBelum ada peringkat
- Insider'S Guide Special Topic: The FDM Approach To Auto-Immune ConditionsDokumen56 halamanInsider'S Guide Special Topic: The FDM Approach To Auto-Immune Conditionssam100% (1)
- Immunity: 1 Line of Defense 2 Line of Defense 3 Line of DefenseDokumen93 halamanImmunity: 1 Line of Defense 2 Line of Defense 3 Line of Defensetaylor449Belum ada peringkat
- Antibody Structure and Function: Parham - Chapter 2Dokumen66 halamanAntibody Structure and Function: Parham - Chapter 2Vishnu Reddy Vardhan PulimiBelum ada peringkat
- Antibody Structure & Function AtfDokumen6 halamanAntibody Structure & Function Atfnofov45585Belum ada peringkat
- Immunoglobulin ADokumen7 halamanImmunoglobulin AsuperlalacuteBelum ada peringkat
- ANTIBODY STRUCTURE AND FUNCTION Year 1 (1) - 2Dokumen22 halamanANTIBODY STRUCTURE AND FUNCTION Year 1 (1) - 2Sindhu BabuBelum ada peringkat
- Candida Tests - Ten Methods To Test For Any Candida OvergrowthDokumen3 halamanCandida Tests - Ten Methods To Test For Any Candida OvergrowthbusinessguyBelum ada peringkat
- Etm 20 6 9260 PDFDokumen7 halamanEtm 20 6 9260 PDFLina UkagoBelum ada peringkat