Anda mungkin juga menyukai
- Theology and Pipe Smoking - 7pDokumen7 halamanTheology and Pipe Smoking - 7pNeimar HahmeierBelum ada peringkat
- Colloid Nodular GoiterDokumen37 halamanColloid Nodular GoiterLori GeorgeBelum ada peringkat
- BurnsDokumen80 halamanBurnsAlina IlovanBelum ada peringkat
- Massage Format..Dokumen2 halamanMassage Format..Anahita Malhan100% (2)
- Pathophysiology - Rheumatoid ArthritisDokumen1 halamanPathophysiology - Rheumatoid ArthritisAngel FiloteoBelum ada peringkat
- Pathophysiology Schistosomiasis: Table in New WindowDokumen7 halamanPathophysiology Schistosomiasis: Table in New WindowKaren Leigh MagsinoBelum ada peringkat
- Pathophysiology of Acute Gastroenteritis: Perforati-NgDokumen1 halamanPathophysiology of Acute Gastroenteritis: Perforati-NgBryan Voltaire Santos LannuBelum ada peringkat
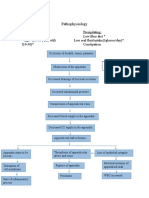
- Appendicitis PathophysiologyDokumen2 halamanAppendicitis PathophysiologyitsmeayaBelum ada peringkat
- Fundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, BhubaneswarDokumen53 halamanFundamentals of Marketing Management: by Prabhat Ranjan Choudhury, Sr. Lecturer, B.J.B (A) College, Bhubaneswarprabhatrc4235Belum ada peringkat
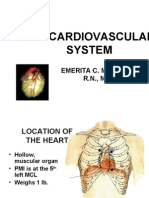
- The Cardiovascular SystemDokumen20 halamanThe Cardiovascular Systembuzz QBelum ada peringkat
- AGE PathophysiologyDokumen1 halamanAGE PathophysiologyZhenmeiBelum ada peringkat
- Stevens Johnson Syndrome CASEDokumen53 halamanStevens Johnson Syndrome CASEKathrina CraveBelum ada peringkat
- Pathophysiology of Bronchial AsthmaDokumen2 halamanPathophysiology of Bronchial AsthmaFirenze Fil100% (21)
- God As CreatorDokumen2 halamanGod As CreatorNeil MayorBelum ada peringkat
- AMOEBIASISDokumen8 halamanAMOEBIASISCheska ت HortelanoBelum ada peringkat
- Amoebiasis Case PresentationDokumen28 halamanAmoebiasis Case Presentationjan micah100% (1)
- Amoebiasis Case StudyDokumen22 halamanAmoebiasis Case StudyChin Villanueva UlamBelum ada peringkat
- BFCDokumen8 halamanBFCIrene GunongBelum ada peringkat
- MeaslesDokumen7 halamanMeaslesKarl FloresBelum ada peringkat
- Case of AmoebiasisDokumen95 halamanCase of Amoebiasisdclaire_1886% (7)
- What Does The Scripture Say - ' - Studies in The Function of Scripture in Early Judaism and Christianity, Volume 1 - The Synoptic GospelsDokumen149 halamanWhat Does The Scripture Say - ' - Studies in The Function of Scripture in Early Judaism and Christianity, Volume 1 - The Synoptic GospelsCometa Halley100% (1)
- NeurologyDokumen42 halamanNeurologybuzz Q100% (2)
- Tetanus PathoDokumen3 halamanTetanus PathoElisha Gine AndalesBelum ada peringkat
- Community Acquired PneumoniaDokumen4 halamanCommunity Acquired PneumoniaKenPedreso100% (2)
- 2018 UPlink NMAT Review Social Science LectureDokumen133 halaman2018 UPlink NMAT Review Social Science LectureFranchesca LugoBelum ada peringkat
- Care of The NewbornDokumen5 halamanCare of The Newbornbuzz Q100% (2)
- Case Study of LeptospirosisDokumen4 halamanCase Study of Leptospirosisbuzz Q75% (4)
- Assessment of The Skin: Pat Jackson AllenDokumen104 halamanAssessment of The Skin: Pat Jackson Allenbuzz Q100% (4)
- Software Quality Metrics MethodologyDokumen17 halamanSoftware Quality Metrics MethodologySumit RajputBelum ada peringkat
- Age With Moderate Dehydration New 1Dokumen74 halamanAge With Moderate Dehydration New 1Jhade Relleta100% (1)
- Case Study of AsthmaDokumen6 halamanCase Study of Asthmabuzz Q100% (4)
- Case Study On TQMDokumen20 halamanCase Study On TQMshinyshani850% (1)
- Case PresDokumen5 halamanCase PresBeverlyBelum ada peringkat
- Amoebiasis CaseDokumen51 halamanAmoebiasis CaseChristine Karen Ang SuarezBelum ada peringkat
- Case Study of AmoebiasisDokumen16 halamanCase Study of AmoebiasisGlorielle ElvambuenaBelum ada peringkat
- Acute Gastro Enteritis 1Dokumen42 halamanAcute Gastro Enteritis 1MichaelKimDugenia0% (1)
- Project Report On Amazon vs. FlipkartDokumen86 halamanProject Report On Amazon vs. FlipkartDimple100% (3)
- Ugib Case StudyDokumen36 halamanUgib Case StudyRJ MarquezBelum ada peringkat
- Acute Gastroenteritis For PediatricsDokumen12 halamanAcute Gastroenteritis For PediatricsJamila B. MohammadBelum ada peringkat
- Amoebiasis PathophysiologyDokumen3 halamanAmoebiasis PathophysiologyApril CornejoBelum ada peringkat
- Pathophysiology of AmoebiasisDokumen1 halamanPathophysiology of AmoebiasisCathy AcquiatanBelum ada peringkat
- Cellular AberrationDokumen6 halamanCellular AberrationCheysser FerolinoBelum ada peringkat
- Pathophysiology AGEDokumen2 halamanPathophysiology AGEMareeze Hatta100% (1)
- Acute Tonsil Lo PharyngitisDokumen13 halamanAcute Tonsil Lo PharyngitisLj Kma Sañol100% (1)
- A Case Study of RupturedDokumen12 halamanA Case Study of RupturedkisBelum ada peringkat
- Grand Case Study FinalDokumen34 halamanGrand Case Study FinalFenina S. CalmaBelum ada peringkat
- Resource Unit On Hypertension.Dokumen14 halamanResource Unit On Hypertension.Eloina Grace Obrero RuleteBelum ada peringkat
- Group #4: Unit Task #1 (Nursing Research I)Dokumen11 halamanGroup #4: Unit Task #1 (Nursing Research I)AriaBelum ada peringkat
- Gastritis: Signs and SymptomsDokumen11 halamanGastritis: Signs and SymptomsSher KhanBelum ada peringkat
- Amoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byDokumen8 halamanAmoebiasis Is An Infection in The Bowel, Particularly The Colon, Characterized byJamie JunioBelum ada peringkat
- Rabi PurDokumen3 halamanRabi PurDiana Laura LeiBelum ada peringkat
- Drugstudy For ElderlyDokumen14 halamanDrugstudy For ElderlyJenniferP.BarrosoBelum ada peringkat
- Pathophysiology of Acute GastroenteritisDokumen2 halamanPathophysiology of Acute GastroenteritisArlan AbraganBelum ada peringkat
- Amoebiasis Case StudyDokumen12 halamanAmoebiasis Case StudyGrace NazarenoBelum ada peringkat
- Cell Ab ActivitiesDokumen7 halamanCell Ab ActivitiesJanelle Cabida Supnad100% (1)
- Buergers Power PointDokumen16 halamanBuergers Power PointYan VencerBelum ada peringkat
- Pathophysiology VolvulusDokumen2 halamanPathophysiology VolvulusHyacinth Bueser Bondad0% (2)
- AmoebiasisDokumen1 halamanAmoebiasisYakumaBelum ada peringkat
- Acute TonsillopharyngitisDokumen17 halamanAcute TonsillopharyngitisRachel Haide NaravalBelum ada peringkat
- 9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Dokumen2 halaman9 Department of Health - Diabetes Mellitus Prevention and Control Program - 2011-12-23Evelyn Chu Nevado67% (3)
- Pathophysiology of Acute GastroenteritisDokumen1 halamanPathophysiology of Acute GastroenteritisAiza Yee Bacani83% (6)
- Patho DiagramDokumen4 halamanPatho DiagramNielArmstrongBelum ada peringkat
- Diagnostics - Nursing ResponsibilitiesDokumen9 halamanDiagnostics - Nursing ResponsibilitiesCarmellaDawn100% (3)
- Case Study Ugib.Dokumen19 halamanCase Study Ugib.Mary Ann Garcia100% (1)
- Tpo Eo Poa LFDDokumen4 halamanTpo Eo Poa LFDEzra Miguel DarundayBelum ada peringkat
- History of Past and Present IllnessDokumen10 halamanHistory of Past and Present IllnessRenea Joy ArruejoBelum ada peringkat
- Schematic Diagram BA HAP HRDokumen2 halamanSchematic Diagram BA HAP HRMika MinsalanBelum ada peringkat
- Pathophysiology of HypovolemiaDokumen1 halamanPathophysiology of HypovolemiaSheana TmplBelum ada peringkat
- Acute Gastroenteritis With Severe DehydrationDokumen22 halamanAcute Gastroenteritis With Severe DehydrationCess Dunwan100% (1)
- IntroductionDokumen6 halamanIntroductionAnne RiztiaBelum ada peringkat
- AmoebiasisDokumen5 halamanAmoebiasisyondaime268875Belum ada peringkat
- Entamoeba HistolyticaDokumen10 halamanEntamoeba HistolyticaMin-Joo Esther ParkBelum ada peringkat
- RP RPDokumen6 halamanRP RPEliezah RodriguezBelum ada peringkat
- 16 Digestive SystemDokumen4 halaman16 Digestive SystemOribello, Athenna Jae W.Belum ada peringkat
- Plenary 3 Group 13Dokumen122 halamanPlenary 3 Group 13Obet Agung 天Belum ada peringkat
- Anatomy and Physiology of The Digestive SystemDokumen5 halamanAnatomy and Physiology of The Digestive SystemKate Cris TalatagodBelum ada peringkat
- Case Study of Liver CirrhosisDokumen3 halamanCase Study of Liver Cirrhosisbuzz Q100% (1)
- Case Study of DMDokumen6 halamanCase Study of DMbuzz Q0% (1)
- ReadmeDokumen1 halamanReadmebuzz QBelum ada peringkat
- Musical InstrumentsDokumen12 halamanMusical Instrumentsbuzz QBelum ada peringkat
- GUT3Dokumen143 halamanGUT3buzz Q100% (1)
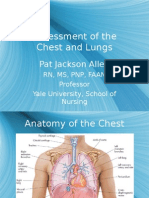
- Assessment of The Chest and Lungs: Pat Jackson AllenDokumen50 halamanAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Growth and DevelopmentDokumen6 halamanGrowth and Developmentbuzz Q100% (3)
- UrologyDokumen28 halamanUrologybuzz QBelum ada peringkat
- Consolidated PCU Labor Law Review 1st Batch Atty Jeff SantosDokumen36 halamanConsolidated PCU Labor Law Review 1st Batch Atty Jeff SantosJannah Mae de OcampoBelum ada peringkat
- Item Bank - Science 5 - 2ND QuarterDokumen11 halamanItem Bank - Science 5 - 2ND QuarterJasmine AguilaBelum ada peringkat
- Pemphigus Subtypes Clinical Features Diagnosis andDokumen23 halamanPemphigus Subtypes Clinical Features Diagnosis andAnonymous bdFllrgorzBelum ada peringkat
- Durability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsDokumen120 halamanDurability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsManjunath ShepurBelum ada peringkat
- Calcutta Bill - Abhimanyug@Dokumen2 halamanCalcutta Bill - Abhimanyug@abhimanyugirotraBelum ada peringkat
- Climate Change Myth or Reality A Critical Analysis of Mainstream English Dailies of India-2019-03!14!09-34Dokumen13 halamanClimate Change Myth or Reality A Critical Analysis of Mainstream English Dailies of India-2019-03!14!09-34Impact JournalsBelum ada peringkat
- Domestic ViolenceDokumen2 halamanDomestic ViolenceIsrar AhmadBelum ada peringkat
- Ped Xi Chapter - 3Dokumen15 halamanPed Xi Chapter - 3DebmalyaBelum ada peringkat
- PDF Document 2Dokumen12 halamanPDF Document 2Nhey VergaraBelum ada peringkat
- Extraction of Non-Timber Forest Products in The PDFDokumen18 halamanExtraction of Non-Timber Forest Products in The PDFRohit Kumar YadavBelum ada peringkat
- BSP Training MatrixDokumen2 halamanBSP Training MatrixLeonisa V. BraganzaBelum ada peringkat
- Afghanistan Law Bibliography 3rd EdDokumen28 halamanAfghanistan Law Bibliography 3rd EdTim MathewsBelum ada peringkat
- Does Moore Succeed in Refuting IdealismDokumen5 halamanDoes Moore Succeed in Refuting IdealismharryBelum ada peringkat
- MC2 Sewing Patterns: Dressmaking Learning ModuleDokumen91 halamanMC2 Sewing Patterns: Dressmaking Learning ModuleMargie JariñoBelum ada peringkat
- Department of Education Division of Cebu ProvinceDokumen5 halamanDepartment of Education Division of Cebu ProvinceNelsie FernanBelum ada peringkat
- Clinical Handbook of Infectious Diseases in Farm AnimalsDokumen146 halamanClinical Handbook of Infectious Diseases in Farm Animalsigorgalopp100% (1)
- Development Communication Theories MeansDokumen13 halamanDevelopment Communication Theories MeansKendra NodaloBelum ada peringkat
- Timothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"Dokumen20 halamanTimothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"PACBelum ada peringkat
- Lesson Plan 2 Revised - Morgan LegrandDokumen19 halamanLesson Plan 2 Revised - Morgan Legrandapi-540805523Belum ada peringkat
- 150 Years of PharmacovigilanceDokumen2 halaman150 Years of PharmacovigilanceCarlos José Lacava Fernández100% (1)