Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- BMS Essay 2Dokumen2 halamanBMS Essay 2Amiera AmaniBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Master Copy Utopia LMT 2022 - Ut 0121 - LaborDokumen11 halamanMaster Copy Utopia LMT 2022 - Ut 0121 - LaborChristian TajarrosBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Live Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Dokumen44 halamanLive Leak - SSC CGL Tier II English Model Question Paper (Based On Predicted Pattern 2016)Testbook BlogBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Siva Siddamsetty Mar PayslipsDokumen1 halamanSiva Siddamsetty Mar PayslipsMaheshSrikakulamBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- WWW NaukrigulfDokumen12 halamanWWW NaukrigulfDesai NileshBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
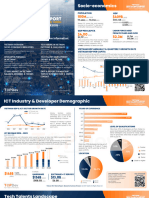
- TopDev VietnamITMarketReport2023 VietnamTechTalentsReport SummaryDokumen5 halamanTopDev VietnamITMarketReport2023 VietnamTechTalentsReport SummaryneitcouqBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Mridc - VN - 31 - Manager - Asst. Manager - Sr. Executive (Civil)Dokumen4 halamanMridc - VN - 31 - Manager - Asst. Manager - Sr. Executive (Civil)Shashank BahiratBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- (FreeCourseWeb - Com) ForeignAffairs01.022020 PDFDokumen208 halaman(FreeCourseWeb - Com) ForeignAffairs01.022020 PDFTiosavBelum ada peringkat
- 第九章 不可抗力事件下允许延长交船日期Dokumen69 halaman第九章 不可抗力事件下允许延长交船日期张为国国际法兴趣小组(2023)Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- 4 Local Government in TexasDokumen63 halaman4 Local Government in TexasNida MahmoodBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Builder - Jan 2015Dokumen190 halamanBuilder - Jan 2015Ashok Subramaniyan100% (1)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Bata Store Manager JD 2019Dokumen2 halamanBata Store Manager JD 2019asgari sheikhBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- CANELA Learning Activity - NSPE Code of EthicsDokumen4 halamanCANELA Learning Activity - NSPE Code of EthicsChristian CanelaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Spence Minera PDFDokumen50 halamanSpence Minera PDFJeral HernándezBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- A Study On Employees Motivation in TANFAC Chemicals Industries Limited Company, CuddaloreDokumen5 halamanA Study On Employees Motivation in TANFAC Chemicals Industries Limited Company, Cuddalorearcherselevators100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- SplicingDokumen111 halamanSplicingamiya001100% (1)
- Bcps Notes 16-17 (II Sem)Dokumen48 halamanBcps Notes 16-17 (II Sem)karamthota bhaskar naikBelum ada peringkat
- MAF Notes Mid ExamDokumen8 halamanMAF Notes Mid ExamPenguin Da Business GooseBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Kalyan Gurukul - Write UpDokumen4 halamanKalyan Gurukul - Write UpArun Kumar SinghBelum ada peringkat
- Envoy Filing H1B Onboarding GuideDokumen11 halamanEnvoy Filing H1B Onboarding GuideRamesh Babu PindigantiBelum ada peringkat
- PH Resorts Customer SatisfactionDokumen22 halamanPH Resorts Customer Satisfactionjoseph lu78% (9)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- WGHRD-14 Summary of ProceedingsDokumen170 halamanWGHRD-14 Summary of ProceedingsAsian Development Bank ConferencesBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Int Bus. IntroDokumen34 halamanInt Bus. IntroShweta SharmaBelum ada peringkat
- Pfizer v. Velasco, March 9, 2011Dokumen2 halamanPfizer v. Velasco, March 9, 2011Isay YasonBelum ada peringkat
- G.R. No. L-6339 April 20, 1954 Manuel Lara, Et Al., Plaintiffs-Appellants, vs. Petronilo Del Rosario, JR., Defendant-Appellee. MontemayorDokumen11 halamanG.R. No. L-6339 April 20, 1954 Manuel Lara, Et Al., Plaintiffs-Appellants, vs. Petronilo Del Rosario, JR., Defendant-Appellee. MontemayorBayani KamporedondoBelum ada peringkat
- Business Brief - Ford Motor CompanyDokumen4 halamanBusiness Brief - Ford Motor CompanyEsther KakaiBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Tips To Increase Employee ProductivityDokumen9 halamanTips To Increase Employee ProductivityedukhojindiaBelum ada peringkat
- UAE Labour LawDokumen23 halamanUAE Labour LawKhuram MunibBelum ada peringkat
- Please Fill The Form in "BLOCK Letters" and Ensure NO Field Is Left BlankDokumen2 halamanPlease Fill The Form in "BLOCK Letters" and Ensure NO Field Is Left BlankcognibpsBelum ada peringkat
- Offer Letter Sasken PankajDokumen12 halamanOffer Letter Sasken PankajLingaiah Chowdary Abburi67% (3)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)