Anda mungkin juga menyukai
- Health Advice and Immunizations for TravelersDari EverandHealth Advice and Immunizations for TravelersBelum ada peringkat
- Pediatric Primary CareDokumen66 halamanPediatric Primary Carefairwoods100% (1)
- Measles and Measles Vaccine Epidemiology and PreventionDokumen18 halamanMeasles and Measles Vaccine Epidemiology and PreventionMar OrdanzaBelum ada peringkat
- Infectious Rubella-4 (Muhadharaty)Dokumen5 halamanInfectious Rubella-4 (Muhadharaty)dr.salam.hassaniBelum ada peringkat
- Iap Guide Book On Immunization Immunization in Special Situations PDFDokumen8 halamanIap Guide Book On Immunization Immunization in Special Situations PDFGirdhari Lal Saini100% (1)
- Pediatric HIV/AIDS: Transmission, Clinical Presentation and ManagementDokumen60 halamanPediatric HIV/AIDS: Transmission, Clinical Presentation and Managementmy Lord JesusBelum ada peringkat
- Immunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheDokumen18 halamanImmunization and Prophylaxis: Childhood Immunization Has Reduced The Impact - Active Immunization Is TheCabdiBelum ada peringkat
- ImmunizationDokumen60 halamanImmunizationleekabrams11Belum ada peringkat
- CPG on Immunization for WomenDokumen28 halamanCPG on Immunization for WomenYnoli DiosomitoBelum ada peringkat
- Immunization Review GPDokumen46 halamanImmunization Review GPKishore ChandkiBelum ada peringkat
- Dr. Ali's Uworld Notes For Step 2 CKDokumen30 halamanDr. Ali's Uworld Notes For Step 2 CKuyesBelum ada peringkat
- Updates in Iraq national immunization program adds rotavirus vaccineDokumen36 halamanUpdates in Iraq national immunization program adds rotavirus vaccineHusain TamimieBelum ada peringkat
- 1 CombineDokumen726 halaman1 CombineSong Hành Vạn KiếpBelum ada peringkat
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDokumen35 halamanImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiBelum ada peringkat
- PAIDSDokumen85 halamanPAIDSw8hxmsvmfzBelum ada peringkat
- DR - Dinesh AgarwalDokumen20 halamanDR - Dinesh AgarwalPushpanjali Crosslay HospitalBelum ada peringkat
- Human Immunodeficiency Virus (Hiv) : Presenter-Dr. Shasidhar ReddyDokumen81 halamanHuman Immunodeficiency Virus (Hiv) : Presenter-Dr. Shasidhar ReddyshravaniBelum ada peringkat
- Malaria & ComorbidDokumen33 halamanMalaria & ComorbidSisilia AlfinaBelum ada peringkat
- Adult ImmunizationDokumen6 halamanAdult ImmunizationAmit GoelBelum ada peringkat
- VaccinationDokumen64 halamanVaccinationnancymhd99Belum ada peringkat
- Vaccination For PregnantDokumen126 halamanVaccination For Pregnantfenan sollanoBelum ada peringkat
- Polio and Polio VaccineDokumen34 halamanPolio and Polio Vaccinevivekmalik420Belum ada peringkat
- Varicella (Chickenpox) Disease: Chananart Yuakyen: IcnDokumen28 halamanVaricella (Chickenpox) Disease: Chananart Yuakyen: IcnKana FajarBelum ada peringkat
- 2 Mumps, RubellaDokumen35 halaman2 Mumps, Rubellaمصطفى رسول هاديBelum ada peringkat
- Pediatric ImmunizationDokumen33 halamanPediatric ImmunizationAlaa Rached Khalid AlmekdadBelum ada peringkat
- Influenza (Flu) Vaccine: DR Vineet Jain Pushpanjali Crosslay HospitalDokumen24 halamanInfluenza (Flu) Vaccine: DR Vineet Jain Pushpanjali Crosslay HospitalPushpanjali Crosslay HospitalBelum ada peringkat
- Pediatric Hiv/Aids: Kussia.A (MD)Dokumen62 halamanPediatric Hiv/Aids: Kussia.A (MD)Yemata HailuBelum ada peringkat
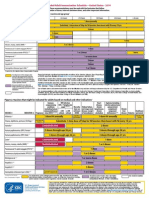
- Childhood Immunization ScheduleDokumen59 halamanChildhood Immunization SchedulejaehankimBelum ada peringkat
- Measles, Mumps and RubellaDokumen45 halamanMeasles, Mumps and RubellaKURBULDKBelum ada peringkat
- Herpes ZosterDokumen26 halamanHerpes ZosterFajar AbdurrahmanBelum ada peringkat
- 1-Measles (Rubeola) PDFDokumen37 halaman1-Measles (Rubeola) PDFمصطفى رسول هاديBelum ada peringkat
- Intra-Uterine and Perinatal InfectionDokumen72 halamanIntra-Uterine and Perinatal InfectionsabrinaBelum ada peringkat
- WHO PP Varicella Herpes Zoster June2014 PresentationDokumen29 halamanWHO PP Varicella Herpes Zoster June2014 PresentationMicki TaryanBelum ada peringkat
- Adult Schedule 11x17Dokumen2 halamanAdult Schedule 11x17lcmurilloBelum ada peringkat
- Immunization PDFDokumen9 halamanImmunization PDFwel2332Belum ada peringkat
- Almostadoctor - Co.uk-Vaccination Schedule UKDokumen6 halamanAlmostadoctor - Co.uk-Vaccination Schedule UKIbrahim FoondunBelum ada peringkat
- Types of ImmunizationsDokumen21 halamanTypes of Immunizationsmacmactongos100% (6)
- Hiv/ Human Immunodeficiency Virus/Aids-Acquired Immunodeficiency SyndromeDokumen16 halamanHiv/ Human Immunodeficiency Virus/Aids-Acquired Immunodeficiency SyndromeNiña Ricci MtflcoBelum ada peringkat
- Adult ScheduleDokumen3 halamanAdult SchedulelcmurilloBelum ada peringkat
- Ob 1.05 Clinical Practice Guidelines On Immunization For Filipino WomenDokumen7 halamanOb 1.05 Clinical Practice Guidelines On Immunization For Filipino Womenotartil_niman50% (2)
- Section Only Full Guideline Recommendations Only Tables Only Drug Tables OnlyDokumen4 halamanSection Only Full Guideline Recommendations Only Tables Only Drug Tables OnlyKhadar BashaBelum ada peringkat
- Influenza Bhasa InggrisDokumen11 halamanInfluenza Bhasa InggrisandiniBelum ada peringkat
- MKSAP 16 - Infectious DiseaseDokumen340 halamanMKSAP 16 - Infectious DiseaseBacanator75% (4)
- Adult ScheduleDokumen3 halamanAdult ScheduleerilarchiBelum ada peringkat
- HIV and ChildrenDokumen32 halamanHIV and ChildrenzidabyBelum ada peringkat
- HIV in ChildrenDokumen11 halamanHIV in ChildrenVaibhav KrishnaBelum ada peringkat
- Drug Therapy: Patient EducationDokumen2 halamanDrug Therapy: Patient EducationJustine Bianca NayreBelum ada peringkat
- Community Health Nursing (Learning Feedback Diary (LFD #25)Dokumen3 halamanCommunity Health Nursing (Learning Feedback Diary (LFD #25)Angelica Malacay RevilBelum ada peringkat
- HIV in PregnancyDokumen28 halamanHIV in PregnancyRaja100% (1)
- Salmonellosis: Condes Dela Cruz ZapataDokumen31 halamanSalmonellosis: Condes Dela Cruz ZapatafuriouspauBelum ada peringkat
- Kepi Vaccines (2) - Gi - 1Dokumen30 halamanKepi Vaccines (2) - Gi - 1okwadha simionBelum ada peringkat
- Varicella and Varicella VaccineDokumen37 halamanVaricella and Varicella VaccineAmudhan MurugesanBelum ada peringkat
- Child Health Program OrientationDokumen143 halamanChild Health Program OrientationKayeBelum ada peringkat
- Immunisation - 4th Yr Feb2022Dokumen49 halamanImmunisation - 4th Yr Feb2022Omar HamwiBelum ada peringkat
- Dr. Elham Bukhari: Aediatri Nfectious IseaseDokumen56 halamanDr. Elham Bukhari: Aediatri Nfectious IseaseJim Jose AntonyBelum ada peringkat
- Pneumococcal Conjugate: VaccineDokumen2 halamanPneumococcal Conjugate: VaccineJenny TaylorBelum ada peringkat
- Multi Vaccine InfantsDokumen3 halamanMulti Vaccine InfantsRahul MukherjeeBelum ada peringkat
- Typhoid and Paratyphoid FeverDokumen17 halamanTyphoid and Paratyphoid FeverGusti ABBelum ada peringkat
- Peds InfectiousDokumen8 halamanPeds InfectiousMohammad RammalBelum ada peringkat
- VXKVNXKVNXKVNXVDokumen1 halamanVXKVNXKVNXKVNXVAbu Furqan FakhrurraziBelum ada peringkat
- JefjsfbswjhwDokumen1 halamanJefjsfbswjhwAbu Furqan FakhrurraziBelum ada peringkat
- OisgishgiosddDokumen1 halamanOisgishgiosddAbu Furqan FakhrurraziBelum ada peringkat
- KJHDJKHDBSDHVBDHJVBDokumen9 halamanKJHDJKHDBSDHVBDHJVBAbu Furqan FakhrurraziBelum ada peringkat
- KGJDKSKFSJDokumen1 halamanKGJDKSKFSJAbu Furqan FakhrurraziBelum ada peringkat
- Hsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikDokumen3 halamanHsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikAbu Furqan FakhrurraziBelum ada peringkat
- KGJDKSKFSJDokumen1 halamanKGJDKSKFSJAbu Furqan FakhrurraziBelum ada peringkat
- KJGSKFSKFMSKDokumen1 halamanKJGSKFSKFMSKAbu Furqan FakhrurraziBelum ada peringkat
- KJKXCBKJBKHXGKDokumen3 halamanKJKXCBKJBKHXGKAbu Furqan FakhrurraziBelum ada peringkat
- Learn about wubfasFHEUIFGASVJSOVHSOVDokumen3 halamanLearn about wubfasFHEUIFGASVJSOVHSOVAbu Furqan FakhrurraziBelum ada peringkat
- Hsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikDokumen4 halamanHsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikAbu Furqan FakhrurraziBelum ada peringkat
- Hsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikDokumen3 halamanHsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikAbu Furqan FakhrurraziBelum ada peringkat
- Wubfasfheuifgasvjsovhsov WubfasfheuifgasvjsovhsovDokumen4 halamanWubfasfheuifgasvjsovhsov WubfasfheuifgasvjsovhsovAbu Furqan FakhrurraziBelum ada peringkat
- Hsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikDokumen8 halamanHsvhdlvhfhblbhsdvnik HsvhdlvhfhblbhsdvnikAbu Furqan FakhrurraziBelum ada peringkat
- The Australian and New Zealand Burn AssociationDokumen97 halamanThe Australian and New Zealand Burn AssociationZarah Alifani Dzulhijjah100% (1)
- Order ReceivedDokumen1 halamanOrder ReceivedAbu Furqan FakhrurraziBelum ada peringkat
- Coping With CaregivingDokumen0 halamanCoping With CaregivingAbu Furqan FakhrurraziBelum ada peringkat
- PediatricsDokumen79 halamanPediatricsapi-3712326Belum ada peringkat
- A Case of Neuromyelitis Optica (Devic's Disease)Dokumen3 halamanA Case of Neuromyelitis Optica (Devic's Disease)Keisha QuinnBelum ada peringkat
- A Case of Neuromyelitis Optica (Devic's Disease)Dokumen3 halamanA Case of Neuromyelitis Optica (Devic's Disease)Keisha QuinnBelum ada peringkat
- Okeechobee County School District 2021-22 Health & Safety ProtocolDokumen3 halamanOkeechobee County School District 2021-22 Health & Safety ProtocolPeterBurkeBelum ada peringkat
- Regents Cells and Human BodyDokumen8 halamanRegents Cells and Human Bodyapi-303120399Belum ada peringkat
- NCM 104 - M6 - DOH Programs Related To Family HealthDokumen4 halamanNCM 104 - M6 - DOH Programs Related To Family HealthJollan Marie Buenvenida0% (1)
- Pneumovax PiDokumen9 halamanPneumovax PipisucamiBelum ada peringkat
- Medicine Update 2021 Section 12Dokumen161 halamanMedicine Update 2021 Section 12Huda AminBelum ada peringkat
- T 249 - RespondentDokumen49 halamanT 249 - Respondentparth singh pariharBelum ada peringkat
- Notification of Vaccination Letter Template: Vaccines AdministeredDokumen1 halamanNotification of Vaccination Letter Template: Vaccines AdministeredJacob BuckBelum ada peringkat
- Poxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Dokumen10 halamanPoxviridae: In: A Concise Review of Veterinary Virology, Carter G.R., Wise D.J. and Flores E.F. (Eds.) - A3410.1005Mestesanu ElisabetaBelum ada peringkat
- Empowerment Technology: Concept Paper ofDokumen2 halamanEmpowerment Technology: Concept Paper ofMary Jane QuijadaBelum ada peringkat
- Global Health Signature Assignment 1Dokumen9 halamanGlobal Health Signature Assignment 1api-534299459Belum ada peringkat
- GCSE Biology - Vaccines - Worksheet AnswersDokumen2 halamanGCSE Biology - Vaccines - Worksheet Answerspangkwan wongprangBelum ada peringkat
- Vaccines - From Concept To Clinic - L. Paoletti, P. McInnes (CRC, 1999) WW PDFDokumen210 halamanVaccines - From Concept To Clinic - L. Paoletti, P. McInnes (CRC, 1999) WW PDFPatriciaBelum ada peringkat
- Reading Practice - 341-408Dokumen68 halamanReading Practice - 341-408El Tea DeeBelum ada peringkat
- MMRDokumen2 halamanMMRShrinivas YuvanBelum ada peringkat
- Emerging Re-Emerging Infectious Disease 2022Dokumen57 halamanEmerging Re-Emerging Infectious Disease 2022marioBelum ada peringkat
- Vaccinations - Dr. Thomas CowanDokumen5 halamanVaccinations - Dr. Thomas Cowanandrogynus71% (7)
- Dr. Ravi MalikDokumen16 halamanDr. Ravi Malikkaabhay8866Belum ada peringkat
- AQA Biol A Unit 3 Jan02Dokumen16 halamanAQA Biol A Unit 3 Jan02woodirocksBelum ada peringkat
- Letter From Doctors To APSDokumen2 halamanLetter From Doctors To APSJustin HinkleyBelum ada peringkat
- Epidemiology and Infection PreventionDokumen32 halamanEpidemiology and Infection Preventionbkbaljeet116131Belum ada peringkat
- Community Medicine GuideDokumen23 halamanCommunity Medicine GuideSohaib Ahmed44% (9)
- HA Drug Formulary - External List v13.4 - 180414Dokumen17 halamanHA Drug Formulary - External List v13.4 - 180414AikBelum ada peringkat
- 980 Final PushDokumen10 halaman980 Final Pushapi-2375055830% (2)
- Protozoa and Fungi Culturing in The LabDokumen7 halamanProtozoa and Fungi Culturing in The LabrorenBelum ada peringkat
- September 9-15, 2012Dokumen24 halamanSeptember 9-15, 2012Bikol ReporterBelum ada peringkat
- Hesc 102Dokumen15 halamanHesc 102Aryansh AryanshBelum ada peringkat
- Jane - Lecture of Typology and Coping IndexDokumen14 halamanJane - Lecture of Typology and Coping IndexArmySapphireBelum ada peringkat
- Assessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationDokumen9 halamanAssessment of Knowledge, Attitudes and Practices of Mothers in Jos North Regarding ImmunizationUlil Amri Pramadani100% (1)
- Vaccine PreservationsDokumen2 halamanVaccine PreservationsAlphonsius WongBelum ada peringkat
- Ethical Issues in HIV Vaccine Trial (Notes)Dokumen63 halamanEthical Issues in HIV Vaccine Trial (Notes)Nuur Mursyiidah MuhammadBelum ada peringkat