Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- DXR Clinician Student User ManualDokumen13 halamanDXR Clinician Student User Manualbjpalmer100% (2)
- Knee PainDokumen32 halamanKnee Painbjpalmer100% (5)
- Ankle ExaminationDokumen16 halamanAnkle Examinationbjpalmer100% (2)
- PhysiotherapyDokumen53 halamanPhysiotherapybjpalmer100% (2)
- DXR Clinician Quick ReferenceDokumen2 halamanDXR Clinician Quick Referencebjpalmer100% (3)
- Gonstead Tech Study SheetDokumen10 halamanGonstead Tech Study Sheetbjpalmer100% (3)
- Medical MnemonicsDokumen256 halamanMedical MnemonicssitalcoolkBelum ada peringkat
- Patellofemoral Pain SyndromeDokumen24 halamanPatellofemoral Pain Syndromebjpalmer100% (3)
- Cortical Dipole and Clinical SignificanceDokumen15 halamanCortical Dipole and Clinical SignificanceManamitaBelum ada peringkat
- BLS Provider Manual PDFDokumen21 halamanBLS Provider Manual PDFAmany Al Mahgoob100% (1)
- Bleuler Psychology PDFDokumen666 halamanBleuler Psychology PDFRicardo Jacobsen Gloeckner100% (2)
- MHD Exam 6 MaterialDokumen179 halamanMHD Exam 6 Materialnaexuis5467100% (1)
- X-Ray-Positioning Spine Dr. FritschDokumen62 halamanX-Ray-Positioning Spine Dr. Fritschbjpalmer100% (3)
- Shortwave Diathermy: 2 Types of Short Wave Diathermy (SWD)Dokumen19 halamanShortwave Diathermy: 2 Types of Short Wave Diathermy (SWD)bjpalmer100% (2)
- Tri 5 Study AidsDokumen698 halamanTri 5 Study Aidsbjpalmer100% (2)
- PostcompsynDokumen3 halamanPostcompsynbjpalmer100% (2)
- SettingsDokumen2 halamanSettingsbjpalmer100% (3)
- Physiotherapy 3Dokumen8 halamanPhysiotherapy 3bjpalmerBelum ada peringkat
- Systems 1 Test 4Dokumen59 halamanSystems 1 Test 4bjpalmer100% (2)
- Pad Placement BookDokumen14 halamanPad Placement Bookbjpalmer100% (2)
- Case Management IDokumen3 halamanCase Management Ibjpalmer100% (2)
- Pediatric Chiro BookDokumen129 halamanPediatric Chiro Bookbjpalmer100% (2)
- ICD Code ChartDokumen1 halamanICD Code ChartbjpalmerBelum ada peringkat
- Lower Leg: Four Fascial CompartmentsDokumen24 halamanLower Leg: Four Fascial Compartmentsbjpalmer100% (2)
- Clinexit GuidelinesDokumen7 halamanClinexit Guidelinesbjpalmer100% (2)
- Tarsal Tunnel SyndromeDokumen7 halamanTarsal Tunnel Syndromebjpalmer100% (2)
- Arthritide Notes OnlyDokumen156 halamanArthritide Notes Onlybjpalmer100% (2)
- Chondromalacia PatellaDokumen5 halamanChondromalacia Patellabjpalmer100% (3)
- B&E (5) Medical BillingDokumen4 halamanB&E (5) Medical Billingbjpalmer100% (2)
- Vascular Disorders and Miscellaneous: Jeffrey R. Thompson, DC, DACBRDokumen43 halamanVascular Disorders and Miscellaneous: Jeffrey R. Thompson, DC, DACBRbjpalmer100% (2)
- WristDokumen11 halamanWristbjpalmer100% (2)
- Skeletal Trauma-Plain Film Trauma Terminology ReviewDokumen35 halamanSkeletal Trauma-Plain Film Trauma Terminology Reviewbjpalmer100% (3)
- Test 1 Review NotesDokumen1 halamanTest 1 Review Notesbjpalmer100% (2)
- SPINEFXDokumen68 halamanSPINEFXbjpalmer100% (2)
- Class10 Nutrition Important Questions 2Dokumen7 halamanClass10 Nutrition Important Questions 2Adarsh SambariBelum ada peringkat
- Diagnostic Exam-Health Specialist EditDokumen9 halamanDiagnostic Exam-Health Specialist EditAyuy Welliss MedusaBelum ada peringkat
- Fluid and Electrolytes BalanceDokumen6 halamanFluid and Electrolytes BalanceMichelle Dona MirallesBelum ada peringkat
- Loco For Cocoa 1 Running Head: LOCO FOR COCOADokumen13 halamanLoco For Cocoa 1 Running Head: LOCO FOR COCOAapi-310439970Belum ada peringkat
- Personal Information Chief Complain History of Presenting IllnessDokumen5 halamanPersonal Information Chief Complain History of Presenting IllnessMuradBelum ada peringkat
- Carlson (7E) : Powerpoint Lecture OutlineDokumen26 halamanCarlson (7E) : Powerpoint Lecture Outlinechat gazaBelum ada peringkat
- The Language, Tone and Prosody of EmotionsDokumen13 halamanThe Language, Tone and Prosody of EmotionsALEJANDRINA VILLAGRAN MONGGIOTTIBelum ada peringkat
- Surgery - RRM PDFDokumen148 halamanSurgery - RRM PDFrajiv peguBelum ada peringkat
- Dental Pulp Stem Cells - Function, Isolation and Applications in Regenerative Medicine PDFDokumen12 halamanDental Pulp Stem Cells - Function, Isolation and Applications in Regenerative Medicine PDFmiguelBelum ada peringkat
- Assessment: Nursing Diagnosis Planning Nursing Interventions Rationale Nursing Care Plan For HypertensionDokumen3 halamanAssessment: Nursing Diagnosis Planning Nursing Interventions Rationale Nursing Care Plan For HypertensionDelaine Mae MierBelum ada peringkat
- The Whole Is Greater Than The Sum of Its PartsDokumen12 halamanThe Whole Is Greater Than The Sum of Its PartsMabelPinesBelum ada peringkat
- Eukaryotic Genome Organisation PDFDokumen2 halamanEukaryotic Genome Organisation PDFKatieBelum ada peringkat
- The Physiology and Habitat of The Last Universal Common AncestorDokumen18 halamanThe Physiology and Habitat of The Last Universal Common AncestorJose MaurtuaBelum ada peringkat
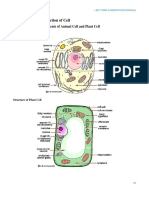
- 1 2 Ultrastructure of Cells - Students NotesDokumen17 halaman1 2 Ultrastructure of Cells - Students Notesapi-289234696Belum ada peringkat
- Foundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokumen19 halamanFoundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralBelum ada peringkat
- 083 41 Final Biologi T4 DLP-30-60Dokumen31 halaman083 41 Final Biologi T4 DLP-30-60Farhan DarwisyBelum ada peringkat
- Worksheet - Respiratory SystemDokumen8 halamanWorksheet - Respiratory SystemDhen MarcBelum ada peringkat
- Plant Tissue Culture (Oreview)Dokumen31 halamanPlant Tissue Culture (Oreview)Aras AfndiiBelum ada peringkat
- Esthetics of Artificial GingivaDokumen13 halamanEsthetics of Artificial GingivaSorabh JainBelum ada peringkat
- Physical Assessment ChecklistDokumen1 halamanPhysical Assessment ChecklistDMRMBelum ada peringkat
- Electrophysiologic Testing EmailDokumen312 halamanElectrophysiologic Testing EmailsafasayedBelum ada peringkat
- Diagnosis and Treatment of Primary AldosteronismDokumen17 halamanDiagnosis and Treatment of Primary AldosteronismcastillojessBelum ada peringkat
- Transport in PlantsDokumen5 halamanTransport in PlantsAlex LochaiBelum ada peringkat
- E01723 Yogic Asanas For Health and Vigour TextDokumen138 halamanE01723 Yogic Asanas For Health and Vigour TextAnonymous nKVk2VC2VEBelum ada peringkat
- Acist Cvi Brochure Us 2014 LRDokumen4 halamanAcist Cvi Brochure Us 2014 LRloulou1306Belum ada peringkat
- Mind Map Sceme Formulation Spem and EggDokumen2 halamanMind Map Sceme Formulation Spem and EggFuzna DahliaBelum ada peringkat