Anda mungkin juga menyukai
- Experimental Thermodynamics: Experimental Thermodynamics of Non-Reacting FluidsDari EverandExperimental Thermodynamics: Experimental Thermodynamics of Non-Reacting FluidsB. Le NeindreBelum ada peringkat
- Ideal Regenerative Rankine Cycle - Closed Feedwater Heaters: Thermodynamics - IIDokumen10 halamanIdeal Regenerative Rankine Cycle - Closed Feedwater Heaters: Thermodynamics - IIsamhameed2Belum ada peringkat
- Engineering Dynamics Lecture 1Dokumen33 halamanEngineering Dynamics Lecture 1Anokha LadlaBelum ada peringkat
- CHAP 3 Gas - Power CyclesDokumen88 halamanCHAP 3 Gas - Power CyclesMuez GhideyBelum ada peringkat
- Thermodynamics h2Dokumen209 halamanThermodynamics h2ezoramajnun100% (1)
- Optimal Rotor Tip Speed RatioDokumen10 halamanOptimal Rotor Tip Speed RatioHaposan YogaBelum ada peringkat
- Carnot CycleDokumen3 halamanCarnot CyclealexontingBelum ada peringkat
- Mechanical Engineering - Course CurriculumDokumen539 halamanMechanical Engineering - Course CurriculumwnaickerBelum ada peringkat
- Me 6301 Engineering Thermodynamics Short Questions and Answers - Unit 2Dokumen7 halamanMe 6301 Engineering Thermodynamics Short Questions and Answers - Unit 2BIBIN CHIDAMBARANATHANBelum ada peringkat
- Chap 5 ThermodynamicsDokumen24 halamanChap 5 ThermodynamicsAsmawi Mohd KhailaniBelum ada peringkat
- Types of BoilersDokumen9 halamanTypes of BoilersAhmad CheemaBelum ada peringkat
- 3.5generation & Transmission of ElectricityDokumen21 halaman3.5generation & Transmission of ElectricityEmil HelmiBelum ada peringkat
- Thermodynamic energy equationDokumen10 halamanThermodynamic energy equationJúlio Gabriel Queiroz dos SantosBelum ada peringkat
- Undergraduate Renewable Energy Course ProjectDokumen24 halamanUndergraduate Renewable Energy Course ProjectAminul HoqueBelum ada peringkat
- Cetane NumberDokumen4 halamanCetane NumberSudarshanBhardwajBelum ada peringkat
- Internal Combustion Engines GuideDokumen16 halamanInternal Combustion Engines GuideAshton SelokaBelum ada peringkat
- First LawDokumen43 halamanFirst Lawviratbansal001Belum ada peringkat
- Power Cycle, Oil, Coal and Natural Gas Introduction To The Rankine Steam Cycle and Carnot EfficiencyDokumen69 halamanPower Cycle, Oil, Coal and Natural Gas Introduction To The Rankine Steam Cycle and Carnot EfficiencyLenin PaudelBelum ada peringkat
- The Second Law of Thermodynamics: Mehmet KanogluDokumen29 halamanThe Second Law of Thermodynamics: Mehmet KanogluDarran Cairns100% (6)
- Tide and Wave EnergyDokumen8 halamanTide and Wave EnergyAnjanKumarDBelum ada peringkat
- Engineering Thermodynamics (LECTURE)Dokumen117 halamanEngineering Thermodynamics (LECTURE)Arvind ArvindBelum ada peringkat
- Chapter 2 - Analysis of Steam Power Plant CycleDokumen61 halamanChapter 2 - Analysis of Steam Power Plant Cyclerrhoshack100% (1)
- Force MeasurementDokumen28 halamanForce MeasurementNaveenKumarMaduri100% (1)
- MS - 57 SolvedDokumen8 halamanMS - 57 Solvedprajwolrajaryal4980Belum ada peringkat
- PHY Chapter 24 The Laws of ThermodynamicsDokumen96 halamanPHY Chapter 24 The Laws of ThermodynamicsAbhishek BansalBelum ada peringkat
- HMT - 2 Marks PDFDokumen29 halamanHMT - 2 Marks PDFFaiyu MechBelum ada peringkat
- Unit I Condction PDFDokumen81 halamanUnit I Condction PDFRishabh AhujaBelum ada peringkat
- Estimation of UncertaintiesDokumen7 halamanEstimation of UncertaintiesNeelMishraBelum ada peringkat
- Air Conditioning System ExperimentDokumen3 halamanAir Conditioning System ExperimentBoJassim100% (1)
- Vdocuments - MX Heat 4e Chap06 LectureDokumen58 halamanVdocuments - MX Heat 4e Chap06 Lecturelarry yimeBelum ada peringkat
- Rankine CycleDokumen9 halamanRankine Cyclewillys8Belum ada peringkat
- THE IDEAL GAS (Topic6)Dokumen18 halamanTHE IDEAL GAS (Topic6)Ted Mana-ayBelum ada peringkat
- PHY203 - Oscillations and WavesDokumen237 halamanPHY203 - Oscillations and WavesMitrabhanuBelum ada peringkat
- Free VibrationsDokumen27 halamanFree Vibrationshelllooo00Belum ada peringkat
- Split-Phase Motor GuideDokumen11 halamanSplit-Phase Motor Guidewensley jethrou guzmanBelum ada peringkat
- Mechanical Engineering BSc Turbo Machinery CourseDokumen4 halamanMechanical Engineering BSc Turbo Machinery CourseLeul SolomonBelum ada peringkat
- BME Unit 1Dokumen40 halamanBME Unit 1Renu PeriketiBelum ada peringkat
- Design, Fabrication and Testing of Human Powered Water PurifierDokumen8 halamanDesign, Fabrication and Testing of Human Powered Water PurifierIJRASETPublicationsBelum ada peringkat
- Mechanical Vibration Week#1 - Elearning VersionDokumen38 halamanMechanical Vibration Week#1 - Elearning VersionBryan PramadiBelum ada peringkat
- Power Plant EngDokumen93 halamanPower Plant Engsenthilkumarece100% (1)
- Chemistry Glossary: Ab Initio (Lat., "From First Principles")Dokumen74 halamanChemistry Glossary: Ab Initio (Lat., "From First Principles")IWantToBelieve8728100% (2)
- Mini Solar Water HeaterDokumen23 halamanMini Solar Water HeaterROCKY DUBEYBelum ada peringkat
- Load Forecasting ClassDokumen24 halamanLoad Forecasting ClassSumit Dhingra100% (1)
- Applied Thermodynamics QBDokumen12 halamanApplied Thermodynamics QBapi-25999517100% (1)
- Adiabatic Flame TemperatureDokumen5 halamanAdiabatic Flame TemperatureRaghav SharmaBelum ada peringkat
- Gas Power Cycles Study Guide in Powerpoint: To AccompanyDokumen68 halamanGas Power Cycles Study Guide in Powerpoint: To AccompanyexceptionalhighdeeBelum ada peringkat
- Chapter 5 - Gas Power CycleDokumen17 halamanChapter 5 - Gas Power CycleIIEC pulchowkBelum ada peringkat
- Thermodynamics GlossaryDokumen1 halamanThermodynamics GlossaryzugoelfinitoBelum ada peringkat
- Oro551 Renewable Energy Sources Syllabus 2.Dokumen2 halamanOro551 Renewable Energy Sources Syllabus 2.Poyyamozhi Nadesan RanjithBelum ada peringkat
- Carnot's Theorem (Thermodynamics) - WikipediaDokumen4 halamanCarnot's Theorem (Thermodynamics) - WikipediaBhuvanesh BalaBelum ada peringkat
- Load CurveDokumen3 halamanLoad Curvesrmce100% (2)
- Mechanical Vibration 2Dokumen2 halamanMechanical Vibration 2Nizar MachmudBelum ada peringkat
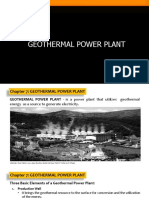
- Chapter 7. Geothermal Power PlantDokumen22 halamanChapter 7. Geothermal Power Plantdiana tahaBelum ada peringkat
- Mbeya Institute of Science and Technology: Power Plant Lecture Seven Hydropower PlantsDokumen125 halamanMbeya Institute of Science and Technology: Power Plant Lecture Seven Hydropower PlantsNyandaMadili MalashiBelum ada peringkat
- Summary, Conclusions, and RecommendationsDokumen2 halamanSummary, Conclusions, and RecommendationsEduBelum ada peringkat
- Bottle Blow Down AnalysisDokumen45 halamanBottle Blow Down AnalysisDoctorOberman100% (2)
- More Energy Efficiency and More Comfort in HospitalsDokumen52 halamanMore Energy Efficiency and More Comfort in HospitalsAlexandr RoscaBelum ada peringkat
- Sustainable Management of Energy ResourcesDokumen4 halamanSustainable Management of Energy ResourcesRaunak Bhansali100% (1)
- Renewable Energy TEE4430 Lecture 5 NotesDokumen9 halamanRenewable Energy TEE4430 Lecture 5 NotesJpricarioBelum ada peringkat
- Innovative Power Distribution For Hospitals PDFDokumen26 halamanInnovative Power Distribution For Hospitals PDFQuophi Click LyfttedBelum ada peringkat
- Steam Users EvolutionDokumen2 halamanSteam Users EvolutionAlexandr RoscaBelum ada peringkat
- Weather SobralDokumen374 halamanWeather SobralAlexandr RoscaBelum ada peringkat
- More Energy Efficiency and More Comfort in HospitalsDokumen52 halamanMore Energy Efficiency and More Comfort in HospitalsAlexandr RoscaBelum ada peringkat
- GUIDELINES For ENERGY EFFICIENCY in HOSPITALSDokumen15 halamanGUIDELINES For ENERGY EFFICIENCY in HOSPITALSAlexandr RoscaBelum ada peringkat
- Dota 2 6.79 Patch NotesDokumen18 halamanDota 2 6.79 Patch NotesAlexandr RoscaBelum ada peringkat
- Large Hospitals 50% Energy SavingsDokumen188 halamanLarge Hospitals 50% Energy SavingsAlexandr RoscaBelum ada peringkat
- Technical Methodology For HospitalDokumen11 halamanTechnical Methodology For HospitalAlexandr RoscaBelum ada peringkat
- GPH Energy Audit Final ReportDokumen120 halamanGPH Energy Audit Final ReportFelipe Andres Moreno BallesterosBelum ada peringkat
- Energy Efficiency in Hospitals (26 Sep 2011)Dokumen0 halamanEnergy Efficiency in Hospitals (26 Sep 2011)Alexandr RoscaBelum ada peringkat
- Energy Audit in HospitalsDokumen47 halamanEnergy Audit in HospitalsAlexandr RoscaBelum ada peringkat
- More Energy Efficiency and More Comfort in HospitalsDokumen52 halamanMore Energy Efficiency and More Comfort in HospitalsAlexandr RoscaBelum ada peringkat
- Predicted Vs Actual Energy Performance of Non Domestic BuildingsDokumen17 halamanPredicted Vs Actual Energy Performance of Non Domestic BuildingsAlexandr RoscaBelum ada peringkat
- Chapter 11 Nuclear StructureDokumen38 halamanChapter 11 Nuclear StructureAimi NabilaBelum ada peringkat
- 4th Generation BiofuelsDokumen5 halaman4th Generation BiofuelsKricel MaqueraBelum ada peringkat
- Petroleum Systems of South Atlantic Marginal BasinsDokumen13 halamanPetroleum Systems of South Atlantic Marginal Basinszulma_anayaBelum ada peringkat
- Wind TB GeneratorDokumen26 halamanWind TB GeneratorbinhBelum ada peringkat
- ME 395 2015 Solutions #4Dokumen2 halamanME 395 2015 Solutions #4me395Belum ada peringkat
- Chicken ManureDokumen2 halamanChicken ManureJuliano, Jhanielle Faye B.Belum ada peringkat
- Answer Key: PHYSICS 1050 Mid-Term Test 2Dokumen8 halamanAnswer Key: PHYSICS 1050 Mid-Term Test 2hey_hopBelum ada peringkat
- Physics 2.2 Mechanics 2-181 To 2-190Dokumen8 halamanPhysics 2.2 Mechanics 2-181 To 2-190siddiqueBelum ada peringkat
- Bremsstrahlung X-RayDokumen2 halamanBremsstrahlung X-RayYuda FhunkshyangBelum ada peringkat
- Chapter 4: Soil Test and SurveyDokumen17 halamanChapter 4: Soil Test and SurveyOpaw Kho100% (1)
- Ped QuestionsDokumen11 halamanPed QuestionsYashPatel100% (1)
- Data Sheet 430W VertexDokumen2 halamanData Sheet 430W VertexErick Rojas JuárezBelum ada peringkat
- OxygenDokumen10 halamanOxygenFaheem HaiderBelum ada peringkat
- Project Proposal CS661Dokumen6 halamanProject Proposal CS661SusovanBelum ada peringkat
- EcologyDokumen50 halamanEcologyKipi Waruku BinisutiBelum ada peringkat
- Activity 9.1: OIL Eeming With IFEDokumen16 halamanActivity 9.1: OIL Eeming With IFEAlisha ChopraBelum ada peringkat
- Bio ScrubberDokumen10 halamanBio ScrubberSata AjjamBelum ada peringkat
- Porosity Measurement Techniques and Applications in Petroleum EngineeringDokumen26 halamanPorosity Measurement Techniques and Applications in Petroleum Engineeringrashed kabbaraBelum ada peringkat
- Chapter 6 - Soil Classification (Aashto & Ucsc)Dokumen33 halamanChapter 6 - Soil Classification (Aashto & Ucsc)Hisham Mohamad100% (2)
- 3 Global Plate TectonicsDokumen29 halaman3 Global Plate TectonicsIvan Bazilije BuhovacBelum ada peringkat
- GR 8 Learning Module in ScienceDokumen6 halamanGR 8 Learning Module in ScienceMaribel100% (1)
- Group 1 ELS FIDPDokumen16 halamanGroup 1 ELS FIDPjayson babaran100% (1)
- Causes of Global Warming: National Geographic SocietyDokumen5 halamanCauses of Global Warming: National Geographic SocietyNahirBelum ada peringkat
- Listen and understand important details from conversations and passagesDokumen3 halamanListen and understand important details from conversations and passagesHa TranBelum ada peringkat
- P 4 Assignment CritiqueDokumen3 halamanP 4 Assignment CritiqueVĩ NguyễnBelum ada peringkat
- Science Process Skills Examination 1ncv0kyDokumen9 halamanScience Process Skills Examination 1ncv0kyInsar Damopolii TempoesekarangBelum ada peringkat
- 2021 Report TotalEnergies Energy LandscapeDokumen126 halaman2021 Report TotalEnergies Energy LandscapeRana Muhammad Ayyaz RasulBelum ada peringkat
- PMC - Module No 11Dokumen17 halamanPMC - Module No 11TALHA ZAFAR72% (50)
- 1 s2.0 S0001868613001140 Main PDFDokumen11 halaman1 s2.0 S0001868613001140 Main PDFBEN DUNCAN MALAGA ESPICHANBelum ada peringkat
- Student Exploration: Air Track: Name: Akshat Date:12/15/20Dokumen9 halamanStudent Exploration: Air Track: Name: Akshat Date:12/15/20Akshat Pant100% (8)