Anda mungkin juga menyukai
- Pediatrics Nutrition 2: Nutritional Disorders Liberiza M. Orseno-Ferrer, MDDokumen9 halamanPediatrics Nutrition 2: Nutritional Disorders Liberiza M. Orseno-Ferrer, MDJill Sanchez-SadiaBelum ada peringkat
- Clinical Nutrition Assessment Form Guidelines Pediatric Ambulatory CareDokumen8 halamanClinical Nutrition Assessment Form Guidelines Pediatric Ambulatory CarePriscilla Okrobea AwukuBelum ada peringkat
- Anthropometry 130824161551 Phpapp02Dokumen48 halamanAnthropometry 130824161551 Phpapp02cuckoo1234Belum ada peringkat
- Critical Ill PDFDokumen5 halamanCritical Ill PDFAnish H DaveBelum ada peringkat
- Kuliah Blok Growth and DevelopmentDokumen44 halamanKuliah Blok Growth and Developmentjaish8904Belum ada peringkat
- Medical Nutrition Therapy For Paediatric ConditionsDokumen57 halamanMedical Nutrition Therapy For Paediatric ConditionsﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞBelum ada peringkat
- Kwashiorkor PresentationDokumen9 halamanKwashiorkor PresentationSushmitha CarkarineBelum ada peringkat
- Protein Energy Malnutrition - M.SC - DAN - 2016 - For ClassDokumen127 halamanProtein Energy Malnutrition - M.SC - DAN - 2016 - For ClassRia Kumar100% (1)
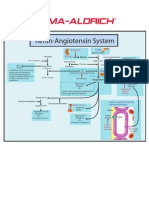
- Renin-Angiotensin SystemDokumen1 halamanRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Congenital SyphilisDokumen6 halamanCongenital SyphilisFrozen Pandora MahayaBelum ada peringkat
- Disease PEMDokumen16 halamanDisease PEMMeena KoushalBelum ada peringkat
- TPNDokumen56 halamanTPNdenekeBelum ada peringkat
- Nutrition & Bio-Chemistry PDFDokumen10 halamanNutrition & Bio-Chemistry PDFRãj Pôtti ÑâîkBelum ada peringkat
- Malnutrition Morris Adams MDokumen31 halamanMalnutrition Morris Adams Mokwadha simionBelum ada peringkat
- Parenteral Nutrition (PN) Clinical and Practical Considerations - CompressedDokumen53 halamanParenteral Nutrition (PN) Clinical and Practical Considerations - CompressedFiya AwanBelum ada peringkat
- Tube FeedingDokumen47 halamanTube FeedingArlyn Mendenilla0% (1)
- Marasmus - Case ReportDokumen13 halamanMarasmus - Case ReportApriany Cordias Arlita SilalahiBelum ada peringkat
- Severe Acute Malnutrition and Fluid Management inDokumen76 halamanSevere Acute Malnutrition and Fluid Management inBibsBelum ada peringkat
- Nutritional Issues in The ICU Case FileDokumen2 halamanNutritional Issues in The ICU Case Filehttps://medical-phd.blogspot.com100% (1)
- Enteral Feeding: Indications, Complications, and Nursing CareDokumen6 halamanEnteral Feeding: Indications, Complications, and Nursing CareSheena CabrilesBelum ada peringkat
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDari EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesBelum ada peringkat
- KwashiorkorDokumen4 halamanKwashiorkorreshma banuBelum ada peringkat
- Management of Severe MalnutritionDokumen77 halamanManagement of Severe Malnutritionfranklin ifioraBelum ada peringkat
- SAMDokumen108 halamanSAMAlimyon Abilar MontoloBelum ada peringkat
- Community Nutrition QuizDokumen3 halamanCommunity Nutrition QuizAli Aufar HutasuhutBelum ada peringkat
- NUTRITIONAL AssessmentDokumen46 halamanNUTRITIONAL AssessmentSonali Hazra0% (1)
- Leprosy CHNDokumen14 halamanLeprosy CHNPhillip ChingBelum ada peringkat
- Growth MonitoringDokumen77 halamanGrowth MonitoringPriti KhemkaBelum ada peringkat
- Prenatal Diagnosis JyDokumen33 halamanPrenatal Diagnosis Jyjien_yeenBelum ada peringkat
- Protocal Followed For Enteral FeedingDokumen4 halamanProtocal Followed For Enteral FeedingK Jayakumar KandasamyBelum ada peringkat
- Case Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Dokumen49 halamanCase Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Izaac JdevBelum ada peringkat
- Toxic Shock Syndrome - PPTX 1-1Dokumen49 halamanToxic Shock Syndrome - PPTX 1-1Mohammed Khedr100% (1)
- NCP RenalDokumen22 halamanNCP Renalمحمود على ما تفرجBelum ada peringkat
- Progress NoteDokumen3 halamanProgress NoteHaji JawaroBelum ada peringkat
- MUMPSDokumen32 halamanMUMPSVer Garcera TalosigBelum ada peringkat
- Failure To ThriveDokumen11 halamanFailure To ThriveFiraFurqaniBelum ada peringkat
- Vitamin B12 Deficiency and A Patient Case StudyDokumen36 halamanVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- 1.1. Protein Energy MalnutritionDokumen13 halaman1.1. Protein Energy MalnutritionAyesha RazzaqBelum ada peringkat
- Kwashiorkor 2Dokumen13 halamanKwashiorkor 2Mutiara Riahna SitepuBelum ada peringkat
- Case Study - NutritionDokumen10 halamanCase Study - NutritionJ.SBelum ada peringkat
- KULDEEP Synopsis Mad by MeDokumen18 halamanKULDEEP Synopsis Mad by MeKuldeep SharmaBelum ada peringkat
- Live Preterm Baby Delivered NSDDokumen13 halamanLive Preterm Baby Delivered NSDKristine Anne SorianoBelum ada peringkat
- Failure To ThriveDokumen3 halamanFailure To Thriveibbs91Belum ada peringkat
- Date Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersDokumen28 halamanDate Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersCm MacaliaBelum ada peringkat
- Pediatric Nursing Care Plan Impaired Physical MobilityDokumen5 halamanPediatric Nursing Care Plan Impaired Physical Mobilityapi-3077327050% (1)
- AssessmentDokumen3 halamanAssessmentchristina lidaBelum ada peringkat
- Chikungunya FeverDokumen15 halamanChikungunya FeverAyomide AlayandeBelum ada peringkat
- Nutrition Support Case StudyDokumen6 halamanNutrition Support Case StudydakotaBelum ada peringkat
- Neonatal Sepsis LectureDokumen142 halamanNeonatal Sepsis Lectureokwadha simion0% (1)
- Parenteral NutritionDokumen8 halamanParenteral NutritionivanBelum ada peringkat
- Meningitis - Introduction and ManagementDokumen27 halamanMeningitis - Introduction and ManagementAmmo KhanBelum ada peringkat
- Article Review Nutrition in Critically Ill ChildDokumen6 halamanArticle Review Nutrition in Critically Ill ChildkhairachungBelum ada peringkat
- PemDokumen30 halamanPemChinchu MohanBelum ada peringkat
- About Creamy LayerDokumen17 halamanAbout Creamy LayerbaluskbBelum ada peringkat
- Hospitalised ChildDokumen7 halamanHospitalised ChildArchana Sahu0% (1)
- Adult Enteral FormulasDokumen2 halamanAdult Enteral FormulasMaulidatul Khasanah New100% (1)
- The Changing Nutritional Needs Across The Life CycleDokumen24 halamanThe Changing Nutritional Needs Across The Life CycleFrance Dave CantorBelum ada peringkat
- PNEUMONIA Case 2 PDFDokumen49 halamanPNEUMONIA Case 2 PDFRed OrangeBelum ada peringkat
- Nutrition For Critically Ill ChildDokumen9 halamanNutrition For Critically Ill Childmalleshwari athramBelum ada peringkat
- Section III ExtraDokumen46 halamanSection III ExtraanurajoneBelum ada peringkat
- Improvement in Documentation of Intake and Output ChartDokumen2 halamanImprovement in Documentation of Intake and Output ChartanurajoneBelum ada peringkat
- Gen Info Intake OutputDokumen3 halamanGen Info Intake OutputanurajoneBelum ada peringkat
- BibliographyDokumen5 halamanBibliographyanurajoneBelum ada peringkat
- Assess Setting Population SampleDokumen1 halamanAssess Setting Population SampleanurajoneBelum ada peringkat
- M.SC FORMATDokumen7 halamanM.SC FORMATanurajoneBelum ada peringkat
- Map Showing Setting of The Study: Nizam Institute of Medical SciencesDokumen1 halamanMap Showing Setting of The Study: Nizam Institute of Medical SciencesanurajoneBelum ada peringkat
- Choanal Atresia1Dokumen5 halamanChoanal Atresia1anurajoneBelum ada peringkat
- Drug ChartDokumen3 halamanDrug ChartanurajoneBelum ada peringkat
- Widenbach TheoryDokumen4 halamanWidenbach TheoryanurajoneBelum ada peringkat
- Informed Consent On DocumentationDokumen3 halamanInformed Consent On DocumentationanurajoneBelum ada peringkat
- Questionnaire On Nursing DocumentationDokumen9 halamanQuestionnaire On Nursing Documentationanurajone92% (13)
- PPTDokumen61 halamanPPTHendra Devandra100% (1)
- BPHM4149 - Chemotherapy-Induced Nausea Vomiting - 22jan2018Dokumen42 halamanBPHM4149 - Chemotherapy-Induced Nausea Vomiting - 22jan2018kkyyyhBelum ada peringkat
- RUNNING HEAD: A Powerful Noise Reflective Essay Mahan 1Dokumen5 halamanRUNNING HEAD: A Powerful Noise Reflective Essay Mahan 1Rachael MahanBelum ada peringkat
- Pathophysiology of Acute GastroenteritisDokumen5 halamanPathophysiology of Acute Gastroenteritisheron_bayanin_15Belum ada peringkat
- Ismail's Undergraduate ThesisDokumen82 halamanIsmail's Undergraduate ThesisAbiola IbrahimBelum ada peringkat
- Burton's Microbiology For The Health Sciences: Chapter 18. Viral InfectionsDokumen20 halamanBurton's Microbiology For The Health Sciences: Chapter 18. Viral Infectionsmirai desu100% (2)
- Health and IllnessDokumen209 halamanHealth and IllnessMeral YünerBelum ada peringkat
- Graded Midterm - Benedictine University EpidemiologyDokumen6 halamanGraded Midterm - Benedictine University EpidemiologyJoshMatthewsBelum ada peringkat
- SyphilisDokumen54 halamanSyphilisYeyeh SantosBelum ada peringkat
- RecentresumeDokumen2 halamanRecentresumeapi-437056180Belum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaNahrijah JahrinaBelum ada peringkat
- Assignment 6 ResumeDokumen1 halamanAssignment 6 Resumeapi-547219401Belum ada peringkat
- Best of Fives For Dentistry 3 ST Ed (2014)Dokumen179 halamanBest of Fives For Dentistry 3 ST Ed (2014)chimedbator100% (3)
- Wound Care Case StudyDokumen5 halamanWound Care Case StudyJulia KennedyBelum ada peringkat
- Acute Febrile IllnessesDokumen96 halamanAcute Febrile IllnessesHAlid mohammed100% (1)
- Library Genesis PDFDokumen8 halamanLibrary Genesis PDFSipra PaulBelum ada peringkat
- Renal Disease in PregnancyDokumen32 halamanRenal Disease in PregnancyHannahKarizaBelum ada peringkat
- De Thi ThuDokumen6 halamanDe Thi ThuQuynh TrangBelum ada peringkat
- Gene Michael Maralit Simundac: ObjectiveDokumen3 halamanGene Michael Maralit Simundac: ObjectiveMary Scarlette CenaBelum ada peringkat
- Flowchart For Assessing Illness in The Absence of The School NurseDokumen1 halamanFlowchart For Assessing Illness in The Absence of The School NurserahkelpBelum ada peringkat
- GMR 2019Dokumen6 halamanGMR 2019arvindat14Belum ada peringkat
- Nurse Labs Practice Test 7 PDFDokumen4 halamanNurse Labs Practice Test 7 PDFNatalie Pemberton-ParrisBelum ada peringkat
- Clinicians Guide To Assessing and Counseling Older Drivers Sep 2020Dokumen282 halamanClinicians Guide To Assessing and Counseling Older Drivers Sep 2020lucia.oliveiraBelum ada peringkat
- Ethics AssignmentDokumen3 halamanEthics Assignmenttonydickpatakesseh100% (4)
- Outline 2Dokumen8 halamanOutline 2api-432489466Belum ada peringkat
- Outline Prog NoteDokumen3 halamanOutline Prog NoteSetya Gon FreccssBelum ada peringkat
- Factors Affecting Patient Safety Culture in A Tertiary Care Hospital in Sri Lanka 1Dokumen8 halamanFactors Affecting Patient Safety Culture in A Tertiary Care Hospital in Sri Lanka 1wawanBelum ada peringkat
- Understanding and Caring For The Person With Dementia: A Practical Guide For CaregiversDokumen40 halamanUnderstanding and Caring For The Person With Dementia: A Practical Guide For CaregiversHadi Najafi100% (2)
- Alternative Therapy in PuerperiumDokumen30 halamanAlternative Therapy in Puerperiumjeny patel100% (6)
- Final Yemen Cmam Guidelines - Feb 2014Dokumen243 halamanFinal Yemen Cmam Guidelines - Feb 2014Anas Abdo SenanBelum ada peringkat