Anda mungkin juga menyukai
- Abcdefghijklmn Opqrstuvwxyz 1234567890Dokumen1 halamanAbcdefghijklmn Opqrstuvwxyz 1234567890Uzzy Lintang SavitriBelum ada peringkat
- Soal Bahasa InggrisDokumen2 halamanSoal Bahasa InggrisUzzy Lintang SavitriBelum ada peringkat
- Asuhan Keperawatan Pada Ker - Int.kul 12Dokumen16 halamanAsuhan Keperawatan Pada Ker - Int.kul 12Uzzy Lintang SavitriBelum ada peringkat
- MobilityDokumen40 halamanMobilityUzzy Lintang SavitriBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Planned Brutality (JM) - T NationDokumen20 halamanPlanned Brutality (JM) - T NationAcclavio33% (3)
- VT TestingDokumen5 halamanVT Testinggogo36Belum ada peringkat
- Chemical and Nutritional Compositions of Flame of Forest (Delonix Regia) Seeds and Seed OilDokumen5 halamanChemical and Nutritional Compositions of Flame of Forest (Delonix Regia) Seeds and Seed OilAbdulrasaq OyedejiBelum ada peringkat
- AtilomataDokumen7 halamanAtilomatamilindBelum ada peringkat
- Modafinil Factsheet (Composite)Dokumen21 halamanModafinil Factsheet (Composite)Danilo ScodellaroBelum ada peringkat
- Genetic Disorders: John W. BachmanDokumen19 halamanGenetic Disorders: John W. BachmannehaBelum ada peringkat
- Intensive V (Complications)Dokumen117 halamanIntensive V (Complications)darren55Belum ada peringkat
- DVT Assessment FormDokumen1 halamanDVT Assessment FormLoy ZiBelum ada peringkat
- Systemic PathologyDokumen21 halamanSystemic PathologyAijan MurzalievaBelum ada peringkat
- OSODROENTDokumen82 halamanOSODROENTAvner TolentinoBelum ada peringkat
- Chapter Two Review of Literature 2.1. Antibacterial ActivityDokumen22 halamanChapter Two Review of Literature 2.1. Antibacterial ActivitywasiuddinBelum ada peringkat
- DS Clarithromycin GI ARLEDDokumen5 halamanDS Clarithromycin GI ARLEDvivi's eyebrowsBelum ada peringkat
- #Comprehensiveclinicalcases #Surgery-Ulcer: Patient ParticularsDokumen5 halaman#Comprehensiveclinicalcases #Surgery-Ulcer: Patient ParticularsRachitha GuttaBelum ada peringkat
- E PortfolioDokumen3 halamanE Portfolioapi-337945337Belum ada peringkat
- D Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsDokumen6 halamanD Kerala PSC Staff Nurse Grade 2 Model Questions Part 4 - Kerala PSC QuestionsMrudula SureshBelum ada peringkat
- Thinking Skills and Problem Solving Oum Jan 2020Dokumen15 halamanThinking Skills and Problem Solving Oum Jan 2020Shoba ManoharanBelum ada peringkat
- Principles of Disease and EpidemiologyR1Dokumen35 halamanPrinciples of Disease and EpidemiologyR1Biancia MckenzieBelum ada peringkat
- Urinary Infections in The ElderlyDokumen29 halamanUrinary Infections in The ElderlyChris FrenchBelum ada peringkat
- Urine Therapy For Any Kind of DiseasesDokumen6 halamanUrine Therapy For Any Kind of DiseasesVipula Parekh60% (5)
- Benchmark Disability As Defined Under Section 2 (R) of The RPWD Act, 2016 and Has LimitationDokumen1 halamanBenchmark Disability As Defined Under Section 2 (R) of The RPWD Act, 2016 and Has LimitationVidhiLegal BlogBelum ada peringkat
- Age ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietDokumen3 halamanAge ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietelleBelum ada peringkat
- Cover Lapkas CAPDokumen1 halamanCover Lapkas CAPRaymond AriantoBelum ada peringkat
- STS100 - That SugarDokumen3 halamanSTS100 - That Sugarbjornebol01Belum ada peringkat
- Genetic Disorder Webquest ArtifactDokumen13 halamanGenetic Disorder Webquest Artifactapi-582653189Belum ada peringkat
- Obesity ICMRDokumen12 halamanObesity ICMRKunalKejriwalBelum ada peringkat
- Schoolarship Exam MCQsDokumen12 halamanSchoolarship Exam MCQsSaber AlasmarBelum ada peringkat
- Neuromuscular ImagingDokumen432 halamanNeuromuscular ImagingLeticiaElizabethEchevarria100% (2)
- Rp0807 - Perform Splinting Techniques Learning ObjectivesDokumen7 halamanRp0807 - Perform Splinting Techniques Learning ObjectivesMuhammad ZubairBelum ada peringkat
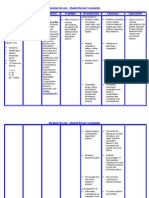
- NURSING CARE PLAN - Liver CirrhosisDokumen2 halamanNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- Racelis Vs United Philippine LinesDokumen1 halamanRacelis Vs United Philippine LinesEarvin Joseph BaraceBelum ada peringkat