Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- FACT SHEET - Efforts To Address Prescription Drug Abuse and Heroin UseDokumen9 halamanFACT SHEET - Efforts To Address Prescription Drug Abuse and Heroin UseurbankimBelum ada peringkat
- ACHC Oakland County FAN Run Drugs Out of Town 2015 ResultsDokumen2 halamanACHC Oakland County FAN Run Drugs Out of Town 2015 ResultsurbankimBelum ada peringkat
- Michigan Association of Community Mental Health Boards 2015 Spring Conference FlyerDokumen5 halamanMichigan Association of Community Mental Health Boards 2015 Spring Conference FlyerurbankimBelum ada peringkat
- Spring Break 2014 Lake Orion StyleDokumen2 halamanSpring Break 2014 Lake Orion StyleurbankimBelum ada peringkat
- Questions and Answers From The Lake Orion Community Mental Health Forum 2/23/2014Dokumen8 halamanQuestions and Answers From The Lake Orion Community Mental Health Forum 2/23/2014urbankimBelum ada peringkat
- Maplegrove 101Dokumen1 halamanMaplegrove 101urbankimBelum ada peringkat
- Summer in The OC 2015Dokumen1 halamanSummer in The OC 2015urbankimBelum ada peringkat
- NOCC Scholoarship Criteria FINAL 2015Dokumen2 halamanNOCC Scholoarship Criteria FINAL 2015urbankimBelum ada peringkat
- Substance Abuse Prevention Ethics TrainingDokumen2 halamanSubstance Abuse Prevention Ethics TrainingurbankimBelum ada peringkat
- Clinical Practice Guidelines As Legal Standards - The Wrong Cure For Health CareDokumen4 halamanClinical Practice Guidelines As Legal Standards - The Wrong Cure For Health CareurbankimBelum ada peringkat
- American Congress of Obstetricians and Gynecologists Support Saving Lives Saving Costs ActDokumen1 halamanAmerican Congress of Obstetricians and Gynecologists Support Saving Lives Saving Costs ActurbankimBelum ada peringkat
- National Consumer Voice For Quality Long Term Care Fact Sheet Financial Exploitation in Nursing HomesDokumen2 halamanNational Consumer Voice For Quality Long Term Care Fact Sheet Financial Exploitation in Nursing HomesurbankimBelum ada peringkat
- Protecting A Loved One From Financial Exploitation in Assisted Living FacilitiesDokumen2 halamanProtecting A Loved One From Financial Exploitation in Assisted Living FacilitiesurbankimBelum ada peringkat
- 1402ReducingPrescriptionDrugAbuse PaperDokumen8 halaman1402ReducingPrescriptionDrugAbuse PaperurbankimBelum ada peringkat
- National Fire Protection Association Turkey Fryer SafetyDokumen1 halamanNational Fire Protection Association Turkey Fryer SafetyurbankimBelum ada peringkat
- Assisted Living Facility Consumer Fact Sheet Financial ExploitationDokumen2 halamanAssisted Living Facility Consumer Fact Sheet Financial Exploitationurbankim0% (1)
- Dr. Aria Sabit ComplaintDokumen18 halamanDr. Aria Sabit ComplainturbankimBelum ada peringkat
- Text Messages To Avoid AlcoholDokumen1 halamanText Messages To Avoid AlcoholurbankimBelum ada peringkat
- Family Day 2013 OffersDokumen1 halamanFamily Day 2013 OffersurbankimBelum ada peringkat
- Dr. Farid Fata FBI HandoutDokumen3 halamanDr. Farid Fata FBI HandouturbankimBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 2019 New Civil ProcedureDokumen47 halaman2019 New Civil ProcedureJayBelum ada peringkat
- Public Officers Sandiganbayan (On Quantum of Evidence)Dokumen16 halamanPublic Officers Sandiganbayan (On Quantum of Evidence)Marjorie Cosares EchavezBelum ada peringkat
- Class Topic: Political Question G.R. No. 196231 January 28, 2014Dokumen2 halamanClass Topic: Political Question G.R. No. 196231 January 28, 2014DEAN JASPERBelum ada peringkat
- NAAIP Valerie B. Jarrett W SignaDokumen3 halamanNAAIP Valerie B. Jarrett W SignaNATIONAL ASSOCIATION for the ADVANCEMENT of INDIGENOUS PEOPLE100% (2)
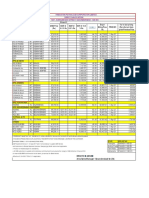
- HPCL PRICE LIST FOR VISAKH, MUMBAI, CHENNAI, VIJAYAWADA AND SECUNDERABAD DEPOTSDokumen1 halamanHPCL PRICE LIST FOR VISAKH, MUMBAI, CHENNAI, VIJAYAWADA AND SECUNDERABAD DEPOTSaee lweBelum ada peringkat
- Digest PP vs. UBIÑADokumen1 halamanDigest PP vs. UBIÑAStef OcsalevBelum ada peringkat
- Concepcion DiaDokumen18 halamanConcepcion DiaChienette MedranoBelum ada peringkat
- Grigoriadis & Özer 2010Dokumen13 halamanGrigoriadis & Özer 2010ehk2Belum ada peringkat
- Senior-citizen tax discounts clarifiedDokumen2 halamanSenior-citizen tax discounts clarifiedJianSadakoBelum ada peringkat
- Obligations and Contracts Fidelity and Deposit Co Vs Wilson 8 Phil 51 January 31, 2020 CASE DIGESTDokumen4 halamanObligations and Contracts Fidelity and Deposit Co Vs Wilson 8 Phil 51 January 31, 2020 CASE DIGESTBrenda de la Gente100% (2)
- Nab McqsDokumen23 halamanNab McqsIzzat FatimaBelum ada peringkat
- Consitution - Meaning, Need, TypesDokumen20 halamanConsitution - Meaning, Need, TypesJoseph MondomaBelum ada peringkat
- Manlapaz Vs CADokumen2 halamanManlapaz Vs CAPatrick James TanBelum ada peringkat
- Gamogamo vs. PNOC Shipping and Transport Corp., 381 SCRA 742 (2002Dokumen16 halamanGamogamo vs. PNOC Shipping and Transport Corp., 381 SCRA 742 (2002Mei SuyatBelum ada peringkat
- Wells - Russia and The Franco-Prussian WarDokumen6 halamanWells - Russia and The Franco-Prussian WarLorena PopescuBelum ada peringkat
- History Class 9 FRENCH REVOLUTIONDokumen18 halamanHistory Class 9 FRENCH REVOLUTIONAngadBelum ada peringkat
- Rappler, editor guilty cyberlibel businessman articleDokumen3 halamanRappler, editor guilty cyberlibel businessman articletaehyung trash100% (2)
- Visayan V NLRCDokumen5 halamanVisayan V NLRCJan Mark WongBelum ada peringkat
- Agenda of The 105th Regular SessionDokumen81 halamanAgenda of The 105th Regular SessionCdeoCityCouncilBelum ada peringkat
- Rule 119 On TrialDokumen5 halamanRule 119 On TrialKaren GinaBelum ada peringkat
- Burgos v. Aquino (Digest)Dokumen2 halamanBurgos v. Aquino (Digest)Patrick DamasoBelum ada peringkat
- Implementasi Rekrutmen CPNS Sebagai Wujud Reformasi Birokrasi Di Kabupaten BogorDokumen14 halamanImplementasi Rekrutmen CPNS Sebagai Wujud Reformasi Birokrasi Di Kabupaten Bogoryohana biamnasiBelum ada peringkat
- Imran Husain Sentencing Memo Oct 2019Dokumen15 halamanImran Husain Sentencing Memo Oct 2019Teri BuhlBelum ada peringkat
- Leyte-Samar Sales Co. vs. Cea and LastrillaDokumen7 halamanLeyte-Samar Sales Co. vs. Cea and LastrillaVeepee PanzoBelum ada peringkat
- ICSI UDIN Guidelines for Certification ServicesDokumen4 halamanICSI UDIN Guidelines for Certification ServicesSACHIN REVEKARBelum ada peringkat
- Netaji-Life & ThoughtsDokumen42 halamanNetaji-Life & ThoughtsVeeresh Gahlot100% (2)
- 17 - Universal Adult Franchise and The Methods of Representation (188 KB)Dokumen9 halaman17 - Universal Adult Franchise and The Methods of Representation (188 KB)Tabish BeighBelum ada peringkat
- Final ObliconDokumen4 halamanFinal ObliconPortgas D. AceBelum ada peringkat
- Faculty of Law 2017/2018Dokumen21 halamanFaculty of Law 2017/2018Juin KerkBelum ada peringkat
- Irr Ra 11917Dokumen92 halamanIrr Ra 11917Virgilio B AberteBelum ada peringkat