Anda mungkin juga menyukai
- Balance Skeletal TractionDokumen3 halamanBalance Skeletal TractionLourdes PinedaBelum ada peringkat
- Orthopedic Nursing LectureDokumen34 halamanOrthopedic Nursing Lecturesjardio100% (2)
- Assisting With Crutchescane or WalkerDokumen11 halamanAssisting With Crutchescane or WalkerJimnah Rhodrick Bontilao100% (1)
- BST ChecklistDokumen3 halamanBST ChecklistBailey100% (1)
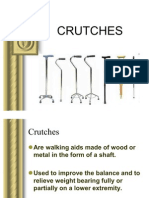
- CRUTCHESDokumen35 halamanCRUTCHESBebing CostinianoBelum ada peringkat
- CrutchesDokumen9 halamanCrutchesEvangel PaduaBelum ada peringkat
- Assistive DevicesDokumen4 halamanAssistive DevicesDandy BongaBelum ada peringkat
- 5.casts and MoldsDokumen30 halaman5.casts and MoldsKatrina PonceBelum ada peringkat
- Cast and TractionsDokumen12 halamanCast and TractionsNoemi Nazareno MarceloBelum ada peringkat
- Splints and Casts Indications and MethodsDokumen9 halamanSplints and Casts Indications and MethodsJay GaneshBelum ada peringkat
- CastDokumen2 halamanCastpoppysmic11Belum ada peringkat
- Braces Ortho..Dokumen16 halamanBraces Ortho..karendelarosa062770% (1)
- Geriatric Assistive DevicesDokumen26 halamanGeriatric Assistive DevicesBrixter Greyson SencronoBelum ada peringkat
- Traction and BracesDokumen1 halamanTraction and BracesCharisse CamantigueBelum ada peringkat
- Cast and BracesDokumen58 halamanCast and BracesNikki M. Arapol100% (1)
- The Balanced Skeletal TractionDokumen1 halamanThe Balanced Skeletal TractionGemarie Adarlo CastilloBelum ada peringkat
- CHN Lecture SY2015-2016 1 SemesterDokumen141 halamanCHN Lecture SY2015-2016 1 SemesterhahahahaaaaaaaBelum ada peringkat
- Principles of Casting and SplintingDokumen8 halamanPrinciples of Casting and Splintingbobtaguba100% (1)
- Ambulation Aids and Assistive DevicesDokumen4 halamanAmbulation Aids and Assistive DevicesDiane Joy Mi-Hi BanaagBelum ada peringkat
- Glasgow Coma ScaleDokumen13 halamanGlasgow Coma ScaleDanna Christine Gumboc PaguntalanBelum ada peringkat
- Fracture (Cast Care)Dokumen6 halamanFracture (Cast Care)Vane UcatBelum ada peringkat
- CastDokumen16 halamanCastSheena Flores Abuga-a100% (1)
- Prepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Dokumen22 halamanPrepared By: Anne Jillian T. Singson, RN, MN: (Assisting Clients in The Use of Assistive Ambulatory Devices)Jan Federick Bantay100% (1)
- Ambulation Aids & Assistive Devices 2007Dokumen109 halamanAmbulation Aids & Assistive Devices 2007Kathrina Ioannou100% (1)
- Ortho BracesDokumen6 halamanOrtho BracesSanny RamosBelum ada peringkat
- Orthopedic NursingDokumen2 halamanOrthopedic NursingMichelle TamorBelum ada peringkat
- Balanced Skeletal TractionDokumen4 halamanBalanced Skeletal TractionOshin Tibangwa Wagayen100% (2)
- Cast and MoldsDokumen11 halamanCast and Moldskaliente0118Belum ada peringkat
- Herniated Nucleus PulposusDokumen17 halamanHerniated Nucleus PulposusCharmaine Joyce Fajardo RosquetaBelum ada peringkat
- Assistive Devices For WalkingDokumen4 halamanAssistive Devices For Walkingthomasfinley44Belum ada peringkat
- Traction NewDokumen37 halamanTraction Newapi-3716867100% (1)
- Hand Hygiene: Alcohol Based Hand RubDokumen2 halamanHand Hygiene: Alcohol Based Hand RubKIERSTINE MARIE BARCELOBelum ada peringkat
- Braces FinalDokumen25 halamanBraces FinalAbigael Patricia Gutierrez100% (1)
- Angelica M. Revil Insight Community Health NursingdocxDokumen2 halamanAngelica M. Revil Insight Community Health NursingdocxAngelica Malacay RevilBelum ada peringkat
- Duties and Responsibilities in or (SCRUB NURSE AND CIRCULATING NURSE) by JheaaDokumen5 halamanDuties and Responsibilities in or (SCRUB NURSE AND CIRCULATING NURSE) by JheaaSareno PJhēaBelum ada peringkat
- Femoral Neck FractureDokumen32 halamanFemoral Neck FractureAndi Karwana Cipta100% (1)
- HNPDokumen7 halamanHNPLyka Mae Imbat - Pacnis100% (1)
- TractionDokumen4 halamanTractionBikram ThapaBelum ada peringkat
- Assisting The Client With Ambulation - CrutchesDokumen4 halamanAssisting The Client With Ambulation - CrutchesKristoffer Castro-DBelum ada peringkat
- Assistive DevicesDokumen3 halamanAssistive DevicesKarina Bianca ColladoBelum ada peringkat
- Use The Following Criteria in Evaluating The Skill PerformanceDokumen4 halamanUse The Following Criteria in Evaluating The Skill Performancekookie100% (1)
- Cast Procedure ChecklistDokumen3 halamanCast Procedure ChecklistEmil A. AquinoBelum ada peringkat
- Cast and Cast CareDokumen3 halamanCast and Cast CareErrol B. Tiozon100% (1)
- Using Mechanical Aids For WalkinDokumen38 halamanUsing Mechanical Aids For Walkinshannon c. lewisBelum ada peringkat
- FractureDokumen8 halamanFractureNica LinsanganBelum ada peringkat
- Surgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingDokumen55 halamanSurgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingCathreen Agatha Fule100% (2)
- Chapter 3 Transferring Patient From Bed To WheelchairDokumen7 halamanChapter 3 Transferring Patient From Bed To Wheelchairdina putri milleniaBelum ada peringkat
- Assistive Devices - WalkerDokumen51 halamanAssistive Devices - WalkerGrand Levi100% (1)
- Application Balanced Skeletal TractionDokumen6 halamanApplication Balanced Skeletal TractionLorenz ChristopherBelum ada peringkat
- Test Questions CA1Dokumen3 halamanTest Questions CA1Gemery Jade ArtatesBelum ada peringkat
- Gastrointestinal SystemDokumen17 halamanGastrointestinal SystempreetBelum ada peringkat
- CIP-NCM-121-Disaster Nursing-TuesdaysDokumen3 halamanCIP-NCM-121-Disaster Nursing-TuesdaysKhen QuiringBelum ada peringkat
- Complete Health AssessmentDokumen3 halamanComplete Health AssessmentQueensterBelum ada peringkat
- IntraoperativeDokumen4 halamanIntraoperativeLynette Roldan RN100% (1)
- Patient Positioning: Complete Guide For MidwivesDokumen12 halamanPatient Positioning: Complete Guide For MidwivesRohlen BaguioBelum ada peringkat
- CC Er Reflection PaperDokumen2 halamanCC Er Reflection Paperapi-545031607Belum ada peringkat
- Unit 10 Activity & ExerciseDokumen110 halamanUnit 10 Activity & ExerciseAshaBelum ada peringkat
- Case StudyDokumen5 halamanCase StudyEdward Jeremy ParasBelum ada peringkat
- Lower Extremity Tractions: Balanced Suspension: Thomas Ring & Pearson & Brady Attachment Buck TractionDokumen22 halamanLower Extremity Tractions: Balanced Suspension: Thomas Ring & Pearson & Brady Attachment Buck TractionJo-Anne Karen SerdeñaBelum ada peringkat
- Assistivedevices 200430182946Dokumen48 halamanAssistivedevices 200430182946Roni's Lifestyle LifeBelum ada peringkat
- Medical-Surgical Nursing (Gastrointestinal)Dokumen1 halamanMedical-Surgical Nursing (Gastrointestinal)アンナドミニクBelum ada peringkat
- Psychiatric NursingDokumen2 halamanPsychiatric NursingアンナドミニクBelum ada peringkat
- Philippine Nursing Licensure Examination May 2014 Requirements and RemindersDokumen2 halamanPhilippine Nursing Licensure Examination May 2014 Requirements and RemindersアンナドミニクBelum ada peringkat
- "Is There a Role for Acupuncture in the Symptom Management of Patients Receiving Palliative Care for Cancer? A Pilot Study of 20 Patients Comparing Acupuncture with Nurse-led Supportive Care" - Journal ReactionDokumen4 halaman"Is There a Role for Acupuncture in the Symptom Management of Patients Receiving Palliative Care for Cancer? A Pilot Study of 20 Patients Comparing Acupuncture with Nurse-led Supportive Care" - Journal ReactionアンナドミニクBelum ada peringkat
- Acute Pain - Nursing Care PlanDokumen9 halamanAcute Pain - Nursing Care Planアンナドミニク89% (37)
- Treatment and Management of Anemia - Teaching PlanDokumen4 halamanTreatment and Management of Anemia - Teaching Planアンナドミニク100% (2)
- Classification of Seizure and Its TypesDokumen6 halamanClassification of Seizure and Its TypesアンナドミニクBelum ada peringkat
- Molar Pregnancy - Case PresentationDokumen7 halamanMolar Pregnancy - Case Presentationアンナドミニク100% (1)
- Infection Control - Teaching PlanDokumen3 halamanInfection Control - Teaching Planアンナドミニク100% (4)
- Deep Breathing and Coughing Exercises - Teaching PlanDokumen3 halamanDeep Breathing and Coughing Exercises - Teaching Planアンナドミニク80% (5)
- Cardiac MuscleDokumen39 halamanCardiac MuscleAndhini Virgiannisa100% (2)
- Esports: The World of Competitive Gaming: An OverviewDokumen19 halamanEsports: The World of Competitive Gaming: An OverviewYeison ChurquipaBelum ada peringkat
- Log 2Dokumen2 halamanLog 2Emanuela MarinescuBelum ada peringkat
- Sompo - Authorised WorkshopsDokumen2 halamanSompo - Authorised WorkshopsWan Ah-LunBelum ada peringkat
- 3 Supporting DetailsDokumen4 halaman3 Supporting Detailsapi-196298078Belum ada peringkat
- Reduction Drive Gear 55,059, C: Disassembly: Automatic TransmissionDokumen3 halamanReduction Drive Gear 55,059, C: Disassembly: Automatic TransmissionAnton FortovBelum ada peringkat
- SIMD Machines:: Pipeline SystemDokumen35 halamanSIMD Machines:: Pipeline Systempssdk99hfdBelum ada peringkat
- Setzi Catalog 2011 2012Dokumen11 halamanSetzi Catalog 2011 2012Angelo Paulo OliveiraBelum ada peringkat
- CauseList PDFDokumen143 halamanCauseList PDFAsif KhanBelum ada peringkat
- Aists 2022 Mas Syllabus - Final VersionDokumen124 halamanAists 2022 Mas Syllabus - Final VersionPrateek Singhal100% (1)
- Water PumpsDokumen5 halamanWater PumpsRachel GrunauerBelum ada peringkat
- Srs V 2Dokumen32 halamanSrs V 2trollergamehuydkBelum ada peringkat
- 7 5 ConnectorsDokumen17 halaman7 5 ConnectorsRonal Quispe HuamanBelum ada peringkat
- Forensic 6 Module - JjbaDokumen71 halamanForensic 6 Module - Jjbabicams02Belum ada peringkat
- FT - Exámenes de Septiembre 2021 - Web 2Dokumen24 halamanFT - Exámenes de Septiembre 2021 - Web 2MATIAS QUINTANABelum ada peringkat
- Data Book: Automotive TechnicalDokumen1 halamanData Book: Automotive TechnicalW̶i̶l̶l̶i̶a̶m̶ Valer Yoi KoeBelum ada peringkat
- Hyatt HotelsDokumen15 halamanHyatt Hotelshttp://www.infoseeds.co.inBelum ada peringkat
- Pre Intermediate Student's Book Answer KeyDokumen53 halamanPre Intermediate Student's Book Answer KeyAna Pociello SamperizBelum ada peringkat
- War Commander Codes UpgradeDokumen2 halamanWar Commander Codes UpgradeRahul Dogra100% (1)
- Abuttment DesignDokumen19 halamanAbuttment DesignHimal KafleBelum ada peringkat
- 3.road MarkingDokumen9 halaman3.road MarkingMalith De SilvaBelum ada peringkat
- Parts Manual - SHG 190 - 2011 ModelDokumen357 halamanParts Manual - SHG 190 - 2011 Modeliqbal hussein100% (3)
- Fallout PNP 4.0 Character SheetDokumen9 halamanFallout PNP 4.0 Character SheetKulakBelum ada peringkat
- B.Inggris Meeting1&2Dokumen4 halamanB.Inggris Meeting1&264212001Belum ada peringkat
- SJG37-2719 PreviewDokumen7 halamanSJG37-2719 PreviewSarah Bronte Connor50% (2)
- Neuromuscular JunctionDokumen16 halamanNeuromuscular JunctionSamadshahirBelum ada peringkat
- ElveonDokumen1 halamanElveonMartin PerušićBelum ada peringkat
- ListeningnExercisen1 695fb5cbe5ed636Dokumen2 halamanListeningnExercisen1 695fb5cbe5ed636sergio luis martinez palaciosBelum ada peringkat
- Michael JordanDokumen10 halamanMichael Jordanapi-534780597Belum ada peringkat
- Amarok - Cacking Noises From Leaf Spring (2030221-3)Dokumen7 halamanAmarok - Cacking Noises From Leaf Spring (2030221-3)DavianGiurcaBelum ada peringkat