Anda mungkin juga menyukai
- Kulit 2 Drug Provocation TesDokumen10 halamanKulit 2 Drug Provocation Tesmrizkidm2301Belum ada peringkat
- 2010 Drug AllergyDokumen78 halaman2010 Drug AllergyEve Methaw100% (1)
- Cleanliness of Bandar Lampung: Oleh: M Rizki Darmawan MDokumen10 halamanCleanliness of Bandar Lampung: Oleh: M Rizki Darmawan Mmrizkidm2301Belum ada peringkat
- Antimicrobial 2013Dokumen82 halamanAntimicrobial 2013Mohammed AbdouBelum ada peringkat
- Generalized Epilepsy With Febrile Seizures-Plus ContextDokumen5 halamanGeneralized Epilepsy With Febrile Seizures-Plus Contextmrizkidm2301Belum ada peringkat
- Handbook: For Clinical Management of DengueDokumen124 halamanHandbook: For Clinical Management of DengueraattaiBelum ada peringkat
- Anak 2Dokumen8 halamanAnak 2mrizkidm2301Belum ada peringkat
- KORTIKOSTEROID Guideline PDFDokumen36 halamanKORTIKOSTEROID Guideline PDFmrizkidm2301Belum ada peringkat
- KORTIKOSTEROID Guideline PDFDokumen36 halamanKORTIKOSTEROID Guideline PDFmrizkidm2301Belum ada peringkat
- Intestinal Parasites OverseasDokumen12 halamanIntestinal Parasites Overseasmrizkidm2301Belum ada peringkat
- Generalized Epilepsy With Febrile Seizures Plus and Classical Idiopathic Generalized EpilepsyDokumen2 halamanGeneralized Epilepsy With Febrile Seizures Plus and Classical Idiopathic Generalized EpilepsyfendysaputraBelum ada peringkat
- Guidelines Focused Update Atrial Fib FTDokumen29 halamanGuidelines Focused Update Atrial Fib FTPanda PavBelum ada peringkat
- Final Presentation EfDokumen11 halamanFinal Presentation Efmrizkidm2301Belum ada peringkat
- Generalized Epilepsy With Febrile Seizures-Plus ContextDokumen5 halamanGeneralized Epilepsy With Febrile Seizures-Plus Contextmrizkidm2301Belum ada peringkat
- Alvarez Hypertension PDFDokumen99 halamanAlvarez Hypertension PDFmeliani.fitriBelum ada peringkat
- Kulit 2 Drug Provocation TesDokumen10 halamanKulit 2 Drug Provocation Tesmrizkidm2301Belum ada peringkat
- Kulit 2 Drug Provocation TesDokumen10 halamanKulit 2 Drug Provocation Tesmrizkidm2301Belum ada peringkat
- 2010 Drug AllergyDokumen78 halaman2010 Drug AllergyEve Methaw100% (1)
- Drug Inducd Skin RX JournalDokumen32 halamanDrug Inducd Skin RX JournalgitarosadilamhBelum ada peringkat
- Impact of Insecticide Resistance On Control of Aedes AegyptiDokumen4 halamanImpact of Insecticide Resistance On Control of Aedes Aegyptimrizkidm2301Belum ada peringkat
- Antimicrobial 2013Dokumen82 halamanAntimicrobial 2013Mohammed AbdouBelum ada peringkat
- p1781 PDFDokumen10 halamanp1781 PDFFrida AnggaBelum ada peringkat
- NIH Stroke ScaleDokumen8 halamanNIH Stroke Scalesridhar100% (2)
- KORTIKOSTEROID Guideline PDFDokumen36 halamanKORTIKOSTEROID Guideline PDFmrizkidm2301Belum ada peringkat
- Final Presentation EfDokumen11 halamanFinal Presentation Efmrizkidm2301Belum ada peringkat
- RabuDokumen1 halamanRabumrizkidm2301Belum ada peringkat
- Cover, Daftar Isi MDokumen3 halamanCover, Daftar Isi Mmrizkidm2301Belum ada peringkat
- Acute Diarrhea Long FINAL 120604Dokumen24 halamanAcute Diarrhea Long FINAL 120604Aizat KamalBelum ada peringkat
- BPH Rico-MussayDokumen16 halamanBPH Rico-Mussaymrizkidm2301Belum ada peringkat
- Oseosarcoma NcbiDokumen4 halamanOseosarcoma Ncbimrizkidm2301Belum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- PBL Biology Infectious DiseaseDokumen11 halamanPBL Biology Infectious Diseaselyana umairahBelum ada peringkat
- LUNGS FunctionsDokumen4 halamanLUNGS FunctionstrinitysugumarBelum ada peringkat
- Frank Clark AutopsyDokumen8 halamanFrank Clark AutopsyK Fine100% (1)
- IS S2 Dictation Notes 21-22Dokumen42 halamanIS S2 Dictation Notes 21-223U09BOWEN DENGBelum ada peringkat
- Respiratory physiology failures and compensationDokumen81 halamanRespiratory physiology failures and compensationMirna HanintyaBelum ada peringkat
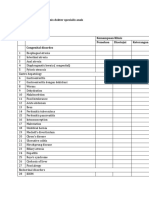
- Rincian Kewenangan Klinis Dokter Spesialis AnakDokumen6 halamanRincian Kewenangan Klinis Dokter Spesialis AnakHikmah AmaliaBelum ada peringkat
- Thoracic TraumaDokumen12 halamanThoracic TraumaNiarti Ulan Sari SiarnuBelum ada peringkat
- 15 Drugs QP Igcse Cie BiologyDokumen7 halaman15 Drugs QP Igcse Cie BiologyHay Thar TunBelum ada peringkat
- 2nd Problem Emergency Medicine Block KEL 1Dokumen141 halaman2nd Problem Emergency Medicine Block KEL 1Jonathan TandajuBelum ada peringkat
- PFT: Assess Lung Function With Pulmonary Function TestsDokumen62 halamanPFT: Assess Lung Function With Pulmonary Function TestsWiz SamBelum ada peringkat
- 7 1 2 B SR Autopsyreporttemplate 6Dokumen4 halaman7 1 2 B SR Autopsyreporttemplate 6api-457390058Belum ada peringkat
- Contorno de Órgão de Risco Thoracic Radiation TherapyDokumen106 halamanContorno de Órgão de Risco Thoracic Radiation TherapyLEONARDO CORDEIRO PEREIRABelum ada peringkat
- ANAPHY Respiratory SystemDokumen30 halamanANAPHY Respiratory SystemAshley Franceska CansanayBelum ada peringkat
- Copd Copd: What Is COPD? Risk FactorsDokumen1 halamanCopd Copd: What Is COPD? Risk FactorsSirikit MaddelaBelum ada peringkat
- Exploratory Laparotomy Post-Op CareDokumen5 halamanExploratory Laparotomy Post-Op CareJaru ObenzaBelum ada peringkat
- MBBS PBL Problems Yr 1-4Dokumen79 halamanMBBS PBL Problems Yr 1-4Keithtra HepburnBelum ada peringkat
- Greys-Anatomy-Student (1) - CompressedDokumen2 halamanGreys-Anatomy-Student (1) - CompressedKaranBelum ada peringkat
- Examination of The Respiratory SystemDokumen12 halamanExamination of The Respiratory SystemChris Jardine LiBelum ada peringkat
- Hasna Arrywn - PART 1Dokumen4 halamanHasna Arrywn - PART 1hasna arrywnBelum ada peringkat
- Estate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Dokumen42 halamanEstate of Jeffrey Scott Lillis v. Correct Care Solutions LLC, Et. Al.Michael_Lee_RobertsBelum ada peringkat
- Short Cases in MedicineDokumen30 halamanShort Cases in MedicineselamuBelum ada peringkat
- Case Study HypertensionDokumen5 halamanCase Study HypertensionPaul Jolo100% (10)
- TB Radiology Basic Presentation SlidesDokumen72 halamanTB Radiology Basic Presentation SlidesSherwin ManuekeBelum ada peringkat
- MGH The Gray Book 2021-2022Dokumen33 halamanMGH The Gray Book 2021-2022Gringo ChanBelum ada peringkat
- Basicinterpretationofcxr 110913060449 Phpapp01Dokumen84 halamanBasicinterpretationofcxr 110913060449 Phpapp01Alexandra DîrțuBelum ada peringkat
- Pediatrics OME + UWORLD NotesDokumen321 halamanPediatrics OME + UWORLD NotesAlenaBelum ada peringkat
- PATHOPHYSIOLOGYDokumen1 halamanPATHOPHYSIOLOGYTri Sha100% (2)
- Síndrome de Insuficiência Torácica Abordagens para Avaliação e TratamentoDokumen7 halamanSíndrome de Insuficiência Torácica Abordagens para Avaliação e TratamentoGuilherme GCBelum ada peringkat
- List of Anatomy Mnemonics - WikipediaDokumen33 halamanList of Anatomy Mnemonics - WikipediaSudeepthiBelum ada peringkat
- QuizDokumen16 halamanQuizDawn MarcoBelum ada peringkat