Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Viral Load SopDokumen18 halamanViral Load SopzamadulaBelum ada peringkat
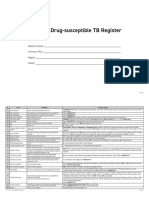
- Form 6a. Drug Susceptible TB RegisterDokumen4 halamanForm 6a. Drug Susceptible TB RegisterAllen ChesterBelum ada peringkat
- Handbook of Oral Diseases 1 Edition PDFDokumen449 halamanHandbook of Oral Diseases 1 Edition PDFEdgar Trujillo Benítez88% (8)
- Digital Transformation of Healthcare at Singapore's Juroaghealth ServiceDokumen3 halamanDigital Transformation of Healthcare at Singapore's Juroaghealth ServiceUsama TahirBelum ada peringkat
- Abhinava ChintamaniDokumen7 halamanAbhinava ChintamaniBrad Yantzer50% (2)
- Bhs Inggris AsthmaDokumen7 halamanBhs Inggris AsthmaAnita nur hidayatiBelum ada peringkat
- Manajemen Pada ObesitasDokumen11 halamanManajemen Pada ObesitasahmadBelum ada peringkat
- Nelmilian Melendez-Garcia 761091 0 1Dokumen6 halamanNelmilian Melendez-Garcia 761091 0 1api-533670449Belum ada peringkat
- XPDokumen290 halamanXPArun Surendran100% (1)
- IELTS Writing Task 1 - Bài Mẫu IELTS FighterDokumen39 halamanIELTS Writing Task 1 - Bài Mẫu IELTS FighterThùyy VyBelum ada peringkat
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDokumen7 halamanSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumBelum ada peringkat
- Paxica - Employee Handbook 08.01.2018Dokumen30 halamanPaxica - Employee Handbook 08.01.2018Jelyn DeseoBelum ada peringkat
- Form 3 Meitheal Planning ReviewDokumen3 halamanForm 3 Meitheal Planning ReviewtqsnrBelum ada peringkat
- LABORATORY SAFETY: A Self-Assessment Workbook - CHAPTERS 1 & 2Dokumen5 halamanLABORATORY SAFETY: A Self-Assessment Workbook - CHAPTERS 1 & 2PA2014Belum ada peringkat
- Container Gardening ManualDokumen12 halamanContainer Gardening ManualApeuDerropBelum ada peringkat
- Morning Report 26 Okt 18Dokumen33 halamanMorning Report 26 Okt 18Nely SilviaBelum ada peringkat
- Uma Kita.: Skylite Musicals 2019 Visual AtmosphereDokumen14 halamanUma Kita.: Skylite Musicals 2019 Visual AtmosphereJasmine AyuBelum ada peringkat
- Removal of CatheterDokumen2 halamanRemoval of CatheterMargaret ArellanoBelum ada peringkat
- Pakistan Orthopaedic Assocition: Memorandum and ArticlesDokumen14 halamanPakistan Orthopaedic Assocition: Memorandum and ArticlesSobia TahirBelum ada peringkat
- Current Challenges With Inflation in NigeriaDokumen23 halamanCurrent Challenges With Inflation in Nigeriajamessabraham2Belum ada peringkat
- KaizenDokumen13 halamanKaizenVlado RadicBelum ada peringkat
- P504 Work PackDokumen16 halamanP504 Work PackFernando SantosBelum ada peringkat
- Ti O2Dokumen4 halamanTi O2Muhamad Fahmi Dermawan EndonesyBelum ada peringkat
- The SkinDokumen5 halamanThe SkinMigvelito219Belum ada peringkat
- Claim ReceiptDokumen3 halamanClaim ReceiptsheerazaliBelum ada peringkat
- What Is Sustainable Development?: Tweet With Us !!Dokumen28 halamanWhat Is Sustainable Development?: Tweet With Us !!clara dupitasBelum ada peringkat
- Vegan. The Healthiest Diet. Henrich, Ernst WalterDokumen42 halamanVegan. The Healthiest Diet. Henrich, Ernst Walteralice1605Belum ada peringkat
- Every Child Matters PDF 2003Dokumen2 halamanEvery Child Matters PDF 2003AshleyBelum ada peringkat
- SOP SMB - 015.3 - Freeze Drying (Martin Christ Machine) GS NC LC 0414Dokumen3 halamanSOP SMB - 015.3 - Freeze Drying (Martin Christ Machine) GS NC LC 0414daizhussain004Belum ada peringkat
- Taryn ZadunayskiDokumen2 halamanTaryn Zadunayskiapi-278580762Belum ada peringkat