Anda mungkin juga menyukai
- Abdominoplasty Classic Principles and TechniqueDokumen18 halamanAbdominoplasty Classic Principles and TechniqueJonathan Zenteno JiménezBelum ada peringkat
- TULUA Springer PDFDokumen10 halamanTULUA Springer PDFCésar Cuadros SerranoBelum ada peringkat
- TULUA Lipoabdominoplasty 2020Dokumen18 halamanTULUA Lipoabdominoplasty 2020Antonio Cardenas100% (1)
- Plastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsDari EverandPlastic & Hand Surgery in Clinical Practice: Classifications and DefinitionsBelum ada peringkat
- Sec 4 - Techniques 2Dokumen31 halamanSec 4 - Techniques 2Karem TubeBelum ada peringkat
- Modified and Radical Neck Dissection TechniqueDokumen19 halamanModified and Radical Neck Dissection TechniquethtklBelum ada peringkat
- The Open Brow LiftDokumen8 halamanThe Open Brow LiftdoctorbanBelum ada peringkat
- 10-16-01 Cleft Lip and Palate Part 1Dokumen52 halaman10-16-01 Cleft Lip and Palate Part 1Zoilo NuñezBelum ada peringkat
- Facial Analysis LRDokumen36 halamanFacial Analysis LRdestiBelum ada peringkat
- Liposuccion Cervical Haack2006Dokumen7 halamanLiposuccion Cervical Haack2006ever renteriaBelum ada peringkat
- Smile Restoration After Facial PalsyDokumen6 halamanSmile Restoration After Facial PalsyJimmie CooperBelum ada peringkat
- LiposuctionDokumen8 halamanLiposuctionnikitagustiBelum ada peringkat
- TULUA Lipoabdominoplasty Transversal Aponeurotic.12Dokumen14 halamanTULUA Lipoabdominoplasty Transversal Aponeurotic.12Carolina Ormaza Giraldo100% (1)
- Ethnic and Gender Considerations in The Use of Facial Injectables: Male PatientsDokumen4 halamanEthnic and Gender Considerations in The Use of Facial Injectables: Male PatientsLuiggi FayadBelum ada peringkat
- Bahan Local FlapDokumen72 halamanBahan Local FlapChandrawati PramanaBelum ada peringkat
- Structural Fat GraftingDokumen19 halamanStructural Fat GraftingGautam KalraBelum ada peringkat
- Manual of Surgery Volume Second: Extremities—Head—Neck. Sixth Edition.Dari EverandManual of Surgery Volume Second: Extremities—Head—Neck. Sixth Edition.Belum ada peringkat
- Plastic SurgeryDokumen6 halamanPlastic SurgeryYing Hui LiewBelum ada peringkat
- Volume Facial e IdadeDokumen6 halamanVolume Facial e IdadeJeniffer RafaelaBelum ada peringkat
- Dr. Rani - Surgical Management of Pressure SoreDokumen19 halamanDr. Rani - Surgical Management of Pressure SoreOtto NaftariBelum ada peringkat
- Auric Recon Slides 070516Dokumen92 halamanAuric Recon Slides 070516Yudhistira AdeBelum ada peringkat
- Facial Nerve Palsy in Newborn PeriodDokumen5 halamanFacial Nerve Palsy in Newborn PeriodjajBelum ada peringkat
- Abdominal Liposuction InstructionDokumen3 halamanAbdominal Liposuction InstructionDizon HenryBelum ada peringkat
- Laser Liposuction Scientific ReseachDokumen31 halamanLaser Liposuction Scientific ReseachBilal HasenBelum ada peringkat
- Tumescent TAPP Laparoscopic Inguinal Hernia RepairDokumen6 halamanTumescent TAPP Laparoscopic Inguinal Hernia RepairUmer KhanBelum ada peringkat
- Gynecomastia Surgery - Power Assisted LiposuctionDokumen4 halamanGynecomastia Surgery - Power Assisted LiposuctionAlfredo Callanta,M.D.Belum ada peringkat
- Reconstructive Conundrums in Dermatologic Surgery: The NoseDari EverandReconstructive Conundrums in Dermatologic Surgery: The NoseDesiree S. RatnerBelum ada peringkat
- Jcad 13 2 33Dokumen11 halamanJcad 13 2 33ntnquynhproBelum ada peringkat
- Complications of BlepharoplastDokumen8 halamanComplications of BlepharoplastdoctorbanBelum ada peringkat
- Update On The Management of Keloids: A. Paul Kelly, MDDokumen6 halamanUpdate On The Management of Keloids: A. Paul Kelly, MDBudi KusumaBelum ada peringkat
- Aesthetic Surgery of The Orbits and EyelidsDokumen31 halamanAesthetic Surgery of The Orbits and EyelidsdoctorbanBelum ada peringkat
- History of RhinoplastyDokumen9 halamanHistory of RhinoplastySyamsul RizalBelum ada peringkat
- Neligan Vol 4 Chapter 10 MainDokumen20 halamanNeligan Vol 4 Chapter 10 MainisabelBelum ada peringkat
- Microsurgical Free FlapsDokumen24 halamanMicrosurgical Free FlapsTaufik Akbar Faried LubisBelum ada peringkat
- Dual Plane ApproachDokumen14 halamanDual Plane ApproachAndreea GhitaBelum ada peringkat
- Flap Selection in Head and Neck Cancer ReconstructionDokumen14 halamanFlap Selection in Head and Neck Cancer ReconstructionFerry RusdiansaputraBelum ada peringkat
- Facial PlasticsDokumen116 halamanFacial Plasticssyed imdadBelum ada peringkat
- Fat Burning Lasers For Surgical Body SculptingDokumen5 halamanFat Burning Lasers For Surgical Body SculptingsrimatsimhasaneshwarBelum ada peringkat
- Kuliah Gangguan Palpebra Dan KonjungtivaDokumen159 halamanKuliah Gangguan Palpebra Dan KonjungtivadudidumBelum ada peringkat
- Asian Rhinoplasty1Dokumen19 halamanAsian Rhinoplasty1drbantmBelum ada peringkat
- Serdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDDokumen4 halamanSerdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDjobetobaBelum ada peringkat
- Aesthetic, Breast 2001 PDFDokumen124 halamanAesthetic, Breast 2001 PDFAhmed AttiaBelum ada peringkat
- BJPS 1984 Cormack Classification of FlapsDokumen8 halamanBJPS 1984 Cormack Classification of FlapsS EllurBelum ada peringkat
- Principles Plastic SurgeryDokumen2 halamanPrinciples Plastic SurgeryIulia DabijaBelum ada peringkat
- Suture Lift and Liposculpture-Chapter 8 PDFDokumen10 halamanSuture Lift and Liposculpture-Chapter 8 PDFAnonymous 8hVpaQdCtrBelum ada peringkat
- Combined Technique of Superficial Liposuction With Ultrasonic Liposculpture PDFDokumen8 halamanCombined Technique of Superficial Liposuction With Ultrasonic Liposculpture PDFeiad-mahmoudBelum ada peringkat
- Congenital Infiltrating Lipomatosis of The Face Case Report PDFDokumen4 halamanCongenital Infiltrating Lipomatosis of The Face Case Report PDFfeli2010Belum ada peringkat
- Aging Facial Skeleton PrsDokumen10 halamanAging Facial Skeleton PrsJorge TreviñoBelum ada peringkat
- A Randomised Controlled Study For The Treatment of Acne Vulgaris Using High Intensity 414nm Solid State Diode ArraysDokumen29 halamanA Randomised Controlled Study For The Treatment of Acne Vulgaris Using High Intensity 414nm Solid State Diode ArraysCaerwyn AshBelum ada peringkat
- Neuromodulators Injection On The ForeheadDokumen24 halamanNeuromodulators Injection On The ForeheadJennifer GomezBelum ada peringkat
- Z-Plasty For Sculpturing of The Bifid Scrotum in Severe Hypospadias Asscociated With Penoscrotal TranspositionDokumen5 halamanZ-Plasty For Sculpturing of The Bifid Scrotum in Severe Hypospadias Asscociated With Penoscrotal TranspositionneonitesBelum ada peringkat
- Emerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Dokumen11 halamanEmerging Trends in Botulinum Neurotoxin A Resistance - An International Multidisciplinary Review and Consensus - Ho, 2022Rafael Autran Cavalcante AraújoBelum ada peringkat
- 2005 Mesotherapy For Body ContouringDokumen5 halaman2005 Mesotherapy For Body ContouringDra. Tatiane FariaBelum ada peringkat
- Integrated Management of The Thick-Skinned Rhinoplasty PatientDokumen6 halamanIntegrated Management of The Thick-Skinned Rhinoplasty PatientFabian Camelo OtorrinoBelum ada peringkat
- 10 16 02CleftLipandPalatePart2 PDFDokumen93 halaman10 16 02CleftLipandPalatePart2 PDFalinutza_childBelum ada peringkat
- Lower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANDokumen3 halamanLower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANHadi FirmansyahBelum ada peringkat
- Nasolabial Flap For Oral Cavity ReconstructionDokumen10 halamanNasolabial Flap For Oral Cavity ReconstructionJamesBelum ada peringkat
- Gox 1 E07 PDFDokumen2 halamanGox 1 E07 PDFUmer HussainBelum ada peringkat
- Alternative Technique For Tip Support in Secondary RhinoplastyDokumen8 halamanAlternative Technique For Tip Support in Secondary RhinoplastydoctorbanBelum ada peringkat
- Laser Skin Treatment in Non-Caucasian PatientsReview ArticleDokumen8 halamanLaser Skin Treatment in Non-Caucasian PatientsReview ArticledoctorbanBelum ada peringkat
- Assessment of Nasal Function After Tip Surgery With A Cephalic Hinged Flap of The Lateral CruraDokumen9 halamanAssessment of Nasal Function After Tip Surgery With A Cephalic Hinged Flap of The Lateral CruradoctorbanBelum ada peringkat
- Are There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemDokumen8 halamanAre There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemdoctorbanBelum ada peringkat
- Ethnic Considerations in Hair Restoration SurgeryReview ArticleDokumen11 halamanEthnic Considerations in Hair Restoration SurgeryReview ArticledoctorbanBelum ada peringkat
- Scar Treatment Variations by Skin TypeReview ArticleDokumen10 halamanScar Treatment Variations by Skin TypeReview ArticledoctorbanBelum ada peringkat
- Repair of A Large Defect of The Upper LipDokumen4 halamanRepair of A Large Defect of The Upper LipdoctorbanBelum ada peringkat
- Microfat Grafting in Nasal SurgeryDokumen17 halamanMicrofat Grafting in Nasal SurgerydoctorbanBelum ada peringkat
- Combined Vestibular Mucosal Advancement and Island Pedicle Flaps For The Repair of A Defect Involving The Cutaneous and Vermilion Upper LipDokumen4 halamanCombined Vestibular Mucosal Advancement and Island Pedicle Flaps For The Repair of A Defect Involving The Cutaneous and Vermilion Upper LipdoctorbanBelum ada peringkat
- Scar Treatment Variations by Skin TypeReview ArticleDokumen10 halamanScar Treatment Variations by Skin TypeReview ArticledoctorbanBelum ada peringkat
- The Role of Gravity in Periorbital andDokumen15 halamanThe Role of Gravity in Periorbital anddoctorbanBelum ada peringkat
- The Pinch Rhytidectomy A Safe, Effective, Low SMAS Variation On The ThemeDokumen17 halamanThe Pinch Rhytidectomy A Safe, Effective, Low SMAS Variation On The ThemedoctorbanBelum ada peringkat
- Repair of A Large Defect of The Upper LipDokumen4 halamanRepair of A Large Defect of The Upper LipdoctorbanBelum ada peringkat
- Are There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemDokumen8 halamanAre There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemdoctorbanBelum ada peringkat
- Repair of A Large Defect of The Upper LipDokumen4 halamanRepair of A Large Defect of The Upper LipdoctorbanBelum ada peringkat
- Are There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemDokumen8 halamanAre There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemdoctorbanBelum ada peringkat
- Comparison Study of Fractional Carbon Dioxide Laser Resurfacing Using Different Fluences and Densities For Acne Scars in AsiansDokumen8 halamanComparison Study of Fractional Carbon Dioxide Laser Resurfacing Using Different Fluences and Densities For Acne Scars in AsiansdoctorbanBelum ada peringkat
- Comparison Study of Fractional Carbon Dioxide Laser Resurfacing Using Different Fluences and Densities For Acne Scars in AsiansDokumen8 halamanComparison Study of Fractional Carbon Dioxide Laser Resurfacing Using Different Fluences and Densities For Acne Scars in AsiansdoctorbanBelum ada peringkat
- Combined Vestibular Mucosal Advancement and Island Pedicle Flaps For The Repair of A Defect Involving The Cutaneous and Vermilion Upper LipDokumen4 halamanCombined Vestibular Mucosal Advancement and Island Pedicle Flaps For The Repair of A Defect Involving The Cutaneous and Vermilion Upper LipdoctorbanBelum ada peringkat
- Are There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemDokumen8 halamanAre There Differences Between The Upper and Lower Parts of The Superficial Musculoaponeurotic SystemdoctorbanBelum ada peringkat
- You Have Full Text Access To This ContentTransient Median and Ulnar Neuropathy Associated With A Microwave Device For Treating Axillary HyperhidrosisDokumen4 halamanYou Have Full Text Access To This ContentTransient Median and Ulnar Neuropathy Associated With A Microwave Device For Treating Axillary HyperhidrosisdoctorbanBelum ada peringkat
- Aging BlepharoplastyDokumen6 halamanAging BlepharoplastydrbantmBelum ada peringkat
- A Simple, Reliable, and Validated Method For Measuring Brow Position.Dokumen5 halamanA Simple, Reliable, and Validated Method For Measuring Brow Position.doctorbanBelum ada peringkat
- The Ulnar Palmar Perforator FlapDokumen7 halamanThe Ulnar Palmar Perforator FlapdoctorbanBelum ada peringkat
- Overlooked Complication ofDokumen9 halamanOverlooked Complication ofdoctorbanBelum ada peringkat
- You Have Full Text Access To This ContentMultimodal Keloid Therapy With Excision, Application of Mitomycin C, and RadiotherapDokumen3 halamanYou Have Full Text Access To This ContentMultimodal Keloid Therapy With Excision, Application of Mitomycin C, and RadiotherapdoctorbanBelum ada peringkat
- The Open Brow LiftDokumen8 halamanThe Open Brow LiftdoctorbanBelum ada peringkat
- Bilobed Flap For Reconstruction of Small Alar Rim DefectsDokumen4 halamanBilobed Flap For Reconstruction of Small Alar Rim DefectsdoctorbanBelum ada peringkat
- Mechanical Analysis of Eyelid MorphologyDokumen9 halamanMechanical Analysis of Eyelid MorphologydoctorbanBelum ada peringkat
- Overlooked Complication ofDokumen9 halamanOverlooked Complication ofdoctorbanBelum ada peringkat
- Community Health Nursing Bag Technique PDFDokumen2 halamanCommunity Health Nursing Bag Technique PDFRachael50% (2)
- Service Delivary Organization Realignment: A Message From Karen Herd, Deputy Minister of Manitoba Health, Seniors and Active LivingDokumen4 halamanService Delivary Organization Realignment: A Message From Karen Herd, Deputy Minister of Manitoba Health, Seniors and Active LivingmatthewtrevithickBelum ada peringkat
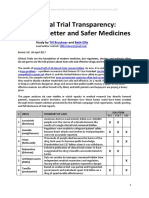
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Dokumen21 halamanClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerBelum ada peringkat
- Practical Standard Prescriber, 7th EditionDokumen505 halamanPractical Standard Prescriber, 7th EditionTonyScaria60% (5)
- What Is Sonography? What Does A Diagnostic Medical Sonographer Do? What Are The Career Opportunities?Dokumen2 halamanWhat Is Sonography? What Does A Diagnostic Medical Sonographer Do? What Are The Career Opportunities?yogimgurtBelum ada peringkat
- Healing TouchDokumen6 halamanHealing TouchDelia Do Rosario100% (1)
- Finalized ResumeDokumen3 halamanFinalized Resumeapi-510470035Belum ada peringkat
- Emergency Protocol ProcedureDokumen14 halamanEmergency Protocol Procedurejmmos207064Belum ada peringkat
- Nclex-Rn Essential Questions and RationalesDokumen96 halamanNclex-Rn Essential Questions and RationalesGloryJane100% (1)
- Latisha Kelly Resume AssignmentDokumen3 halamanLatisha Kelly Resume Assignmentapi-324927307Belum ada peringkat
- Somalia Launches First Ever-Cleft Lip and Palate Surgery ClinicDokumen4 halamanSomalia Launches First Ever-Cleft Lip and Palate Surgery ClinicAMISOM Public Information ServicesBelum ada peringkat
- IsosorbideDokumen2 halamanIsosorbideSBelum ada peringkat
- Comfort Room PDFDokumen1 halamanComfort Room PDFPixaaaBelum ada peringkat
- Know Your Magnetic FieldDokumen75 halamanKnow Your Magnetic FieldAtma Jnani100% (5)
- Basic ECGDokumen152 halamanBasic ECGTuấn Thanh VõBelum ada peringkat
- Liver Function TestDokumen20 halamanLiver Function TestAvi VermaBelum ada peringkat
- Manual of Basic Techniques For A Health Laboratory (Part1) - WHODokumen114 halamanManual of Basic Techniques For A Health Laboratory (Part1) - WHOcholinchuchuBelum ada peringkat
- Nursing Care Plan Breast-CancerDokumen2 halamanNursing Care Plan Breast-CancerGreg Llandelar100% (2)
- Flap HemisoleusDokumen6 halamanFlap HemisoleuscweetblueBelum ada peringkat
- Healthcare System and Reforms in The United States Revised Essay 3Dokumen4 halamanHealthcare System and Reforms in The United States Revised Essay 3api-272097622Belum ada peringkat
- MEdical Surgical REVEWERDokumen86 halamanMEdical Surgical REVEWERennaedBelum ada peringkat
- Infants and Children - Pediatric EmergenciesDokumen27 halamanInfants and Children - Pediatric EmergenciesIlmiah BagusBelum ada peringkat
- CV 2017 VirginiaDokumen4 halamanCV 2017 Virginiaapi-353693776Belum ada peringkat
- FTHHHDokumen17 halamanFTHHHSaad khanBelum ada peringkat
- Final Past Papers With Common MCQS: MedicineDokumen17 halamanFinal Past Papers With Common MCQS: MedicineKasun PereraBelum ada peringkat
- Fingertips Injury: Literature ReviewDokumen24 halamanFingertips Injury: Literature ReviewDonny Artya KesumaBelum ada peringkat
- Ebp PaperDokumen8 halamanEbp Paperapi-250304529Belum ada peringkat
- Hyper Parathyroid IsmDokumen7 halamanHyper Parathyroid IsmEllene Mae Dejapa VillasisBelum ada peringkat
- Guidelines For Prescribing EyeglassesDokumen18 halamanGuidelines For Prescribing Eyeglassesratujelita100% (1)
- Anticoagulants 2019Dokumen11 halamanAnticoagulants 2019Srijan VermaBelum ada peringkat