Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Anatomy and Physiology - Dengue FeverDokumen3 halamanAnatomy and Physiology - Dengue Feverhael yam62% (13)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- SLEDokumen42 halamanSLETrishenth FonsekaBelum ada peringkat
- Synthetic Approach ReportDokumen20 halamanSynthetic Approach ReportMarivic Diano100% (1)
- Return On InvestmentDokumen15 halamanReturn On InvestmentMarivic DianoBelum ada peringkat
- Light of HOPEDokumen33 halamanLight of HOPEMarivic DianoBelum ada peringkat
- Why Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Dokumen2 halamanWhy Did They Hide It FROM US: Remedy That Is 10,000 Times Stronger Than Chemotherapy!Marivic DianoBelum ada peringkat
- Wellness PowerpointDokumen28 halamanWellness PowerpointMarivic Diano0% (1)
- Animal Tissues: Asia Technological School of Science and ArtsDokumen2 halamanAnimal Tissues: Asia Technological School of Science and ArtsMarivic DianoBelum ada peringkat
- BiologyDokumen42 halamanBiologyMarivic DianoBelum ada peringkat
- Under The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsDokumen79 halamanUnder The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsMarivic DianoBelum ada peringkat
- Hospital Incident Command System (HICS) : Reported byDokumen42 halamanHospital Incident Command System (HICS) : Reported byMarivic DianoBelum ada peringkat
- Nurse To Colleagues: You Deserve A Break Today: by Tyler SmithDokumen2 halamanNurse To Colleagues: You Deserve A Break Today: by Tyler SmithMarivic DianoBelum ada peringkat
- Iv Regulation and Controlling DevicesDokumen21 halamanIv Regulation and Controlling DevicesMarivic DianoBelum ada peringkat
- Anatomy and Physiology of BVDokumen16 halamanAnatomy and Physiology of BVMarivic DianoBelum ada peringkat
- Palliative and Terminal CareDokumen78 halamanPalliative and Terminal CareMarivic DianoBelum ada peringkat
- Renal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyDokumen50 halamanRenal Cell Carcinoma - Nursing Considerations With The Use of Targeted TherapyMarivic DianoBelum ada peringkat
- Disaster Risk Management and MitigationDokumen5 halamanDisaster Risk Management and MitigationMarivic DianoBelum ada peringkat
- Suprising Truths About MotivationDokumen2 halamanSuprising Truths About MotivationMarivic DianoBelum ada peringkat
- MeaslesDokumen11 halamanMeaslesMarivic DianoBelum ada peringkat
- Fractures: (On Which We Will Likely Be Pimped)Dokumen66 halamanFractures: (On Which We Will Likely Be Pimped)Marivic DianoBelum ada peringkat
- Nurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsDokumen31 halamanNurses' Perceived Job Related Stress and Job Satisfaction in Amman Private HospitalsMarivic Diano100% (1)
- Fluid and Electrolytes Report!!Dokumen20 halamanFluid and Electrolytes Report!!Marivic DianoBelum ada peringkat
- Cancer Ozone Therapy Treatment A DiscussionDokumen13 halamanCancer Ozone Therapy Treatment A DiscussionjpgbfBelum ada peringkat
- Comorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dokumen10 halamanComorbidity: Apakah Merupakan Faktor Risiko: Infeksi Luka Operasi Pasca Seksio Sesarea?Dini AgustiniBelum ada peringkat
- Secukinumab: First Global ApprovalDokumen10 halamanSecukinumab: First Global ApprovalAri KurniawanBelum ada peringkat
- Wound CareDokumen77 halamanWound CareNestor Balboa100% (1)
- BioavailabilityDokumen35 halamanBioavailabilityDr. Bharat JainBelum ada peringkat
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDokumen12 halamanExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcBelum ada peringkat
- Daftar Jurnal Kedokteran Internasional GratisDokumen3 halamanDaftar Jurnal Kedokteran Internasional GratisdoktermutiaBelum ada peringkat
- Urtricaria SDokumen8 halamanUrtricaria SpalBelum ada peringkat
- Disorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedDokumen25 halamanDisorders of Immunity Hypersensitivity Reactions: Dr. Mehzabin AhmedFrances FranciscoBelum ada peringkat
- DctsDokumen30 halamanDctsInuyashayahoo100% (1)
- Itpc PT ProcessDokumen2 halamanItpc PT ProcessKyle MañiboBelum ada peringkat
- Festival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Dokumen29 halamanFestival Dance Lesson - Module 2 - P.E. 3rd Quarter PPT 2 of 2Maria Fe VibarBelum ada peringkat
- Anxiety: What Are Some Symptoms of Anxiety?Dokumen3 halamanAnxiety: What Are Some Symptoms of Anxiety?Khairil AshrafBelum ada peringkat
- Congestion Pelvica 2020Dokumen6 halamanCongestion Pelvica 2020Cristian RodríguezBelum ada peringkat
- Newborn CareDokumen19 halamanNewborn CareYa Mei LiBelum ada peringkat
- WellCat Veterinary HandbookDokumen36 halamanWellCat Veterinary HandbookKatSiebrecht100% (5)
- DKA Handout1Dokumen59 halamanDKA Handout1aleBelum ada peringkat
- TramadolDokumen2 halamanTramadolJordanne EtisBelum ada peringkat
- 7 AHM Antibiotic PolicyDokumen98 halaman7 AHM Antibiotic PolicyfaisalBelum ada peringkat
- Mental IllnessDokumen3 halamanMental IllnessKate EvangelistaBelum ada peringkat
- Anesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFDokumen125 halamanAnesthesia For The Pet Practitioner (Banfield, 2003 Edition) PDFKatarina SimicicBelum ada peringkat
- Celiac DiseaseDokumen5 halamanCeliac DiseaseJhevey ValdezBelum ada peringkat
- Euthanasia in Experimental AnimalsDokumen22 halamanEuthanasia in Experimental AnimalsParmanand AtalBelum ada peringkat
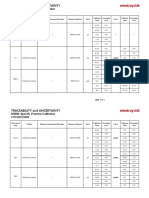
- Specific Proteins Calibrator-150721009-BS600Dokumen2 halamanSpecific Proteins Calibrator-150721009-BS600S6b2Belum ada peringkat
- Icd9 Icd10 Reference SheetDokumen1 halamanIcd9 Icd10 Reference Sheetapi-272182068Belum ada peringkat
- Balance Training For Older Adults.: Daftar PustakaDokumen4 halamanBalance Training For Older Adults.: Daftar PustakatetikBelum ada peringkat
- LaparotomyDokumen36 halamanLaparotomydenekeBelum ada peringkat
- Aneurysm: Symptoms of An AneurysmDokumen3 halamanAneurysm: Symptoms of An AneurysmArun MuralidharanBelum ada peringkat