Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- VP Director Sales in Irvine CA Resume Roy MaderDokumen4 halamanVP Director Sales in Irvine CA Resume Roy MaderRoyMaderBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- 13 Interview Questions and Answers ExamplesDokumen14 halaman13 Interview Questions and Answers ExamplesCarl William Chua100% (1)
- Group 7 - CRISILDokumen12 halamanGroup 7 - CRISILSamhitha AB100% (3)
- Leadership in The 21st CenturyDokumen25 halamanLeadership in The 21st CenturySherif RafikBelum ada peringkat
- Organizational Behaviour Case Incident 2Dokumen5 halamanOrganizational Behaviour Case Incident 2Siti Suhaili Zainal Abidin100% (1)
- Leadership and Management in Pharmacy Practice: Second EditionDokumen99 halamanLeadership and Management in Pharmacy Practice: Second Editionethio mkBelum ada peringkat
- Presentation ERPDokumen23 halamanPresentation ERP9986212378Belum ada peringkat
- Managing Spare PartsDokumen3 halamanManaging Spare PartsPrasad PnBelum ada peringkat
- NSTP OBE Syllabus-GeneralDokumen10 halamanNSTP OBE Syllabus-GeneralYanna Manuel100% (2)
- Upload Kaizen Charter - Form 1 PGDokumen2 halamanUpload Kaizen Charter - Form 1 PGmanuelBelum ada peringkat
- Scrum Foundation Sample ExamDokumen7 halamanScrum Foundation Sample Examr076755aBelum ada peringkat
- Alec Fra HerDokumen12 halamanAlec Fra Heralec fraherBelum ada peringkat
- Unfair Terms of ContractDokumen13 halamanUnfair Terms of Contractalec fraherBelum ada peringkat
- Making Sense of Complex NeedDokumen44 halamanMaking Sense of Complex Needalec fraherBelum ada peringkat
- CQC (v2)Dokumen9 halamanCQC (v2)alec fraherBelum ada peringkat
- Better, Brighter Futures: Approved Preferred Provider SchemeDokumen17 halamanBetter, Brighter Futures: Approved Preferred Provider Schemealec fraherBelum ada peringkat
- Sub-Regional Specialist Category Sourcing Programme: Alec Fraher and Associates LTD June 2008Dokumen30 halamanSub-Regional Specialist Category Sourcing Programme: Alec Fraher and Associates LTD June 2008alec fraherBelum ada peringkat
- SOTW Framework Ed Version)Dokumen6 halamanSOTW Framework Ed Version)alec fraherBelum ada peringkat
- Better Brighter DocDokumen66 halamanBetter Brighter Docalec fraherBelum ada peringkat
- Sotw Road MapDokumen36 halamanSotw Road Mapalec fraherBelum ada peringkat
- Provincial Cooperative and Enterprise Development Office: Republic of The PhilippinesDokumen4 halamanProvincial Cooperative and Enterprise Development Office: Republic of The PhilippinesRoel P. Dolaypan Jr.Belum ada peringkat
- Chap 12 Performance Measurement FINALDokumen14 halamanChap 12 Performance Measurement FINALOnkar SawantBelum ada peringkat
- Culture Playbook - v2 - FINALDokumen28 halamanCulture Playbook - v2 - FINALEstela CarrilloBelum ada peringkat
- Culture & Strategy: Chris KariyawasamDokumen43 halamanCulture & Strategy: Chris KariyawasamSandyBelum ada peringkat
- Block 4 MCO 1 Unit 1Dokumen23 halamanBlock 4 MCO 1 Unit 1Tushar SharmaBelum ada peringkat
- Succi, C., & Canovi, M. (2020)Dokumen15 halamanSucci, C., & Canovi, M. (2020)kellymeinhold327Belum ada peringkat
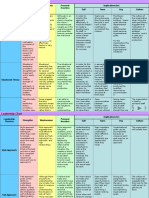
- Leadership Theories Strengths: Weaknesses: Personal Reaction Implications For: Self Team Org CultureDokumen2 halamanLeadership Theories Strengths: Weaknesses: Personal Reaction Implications For: Self Team Org CulturedrengerguriBelum ada peringkat
- Unit 2 Interviewing ProjectDokumen18 halamanUnit 2 Interviewing Projectapi-561601258Belum ada peringkat
- Avi R. Chaudhary - Cover Letter (PWC)Dokumen1 halamanAvi R. Chaudhary - Cover Letter (PWC)prashant mishraBelum ada peringkat
- HRM101 Ch1Dokumen41 halamanHRM101 Ch1Basheer Al-GhazaliBelum ada peringkat
- 7010 - Sample AssignmnetDokumen24 halaman7010 - Sample AssignmnetSh Hirra Tahir100% (2)
- SYLLLAB - Strategic ManagementDokumen14 halamanSYLLLAB - Strategic ManagementEfrenBelum ada peringkat
- ProjectDokumen42 halamanProjectNikhil BirajBelum ada peringkat
- Strategic Planning and Human ResourcesDokumen6 halamanStrategic Planning and Human ResourcesSolutions MasterBelum ada peringkat
- Synopsis On Employee SatisfactionDokumen8 halamanSynopsis On Employee SatisfactionPrasenjit BiswasBelum ada peringkat
- Islamophobia Case StudyDokumen17 halamanIslamophobia Case StudyFlixBelum ada peringkat
- Perancangan Sistem Informasi Logistik Dan Basis Data: ILI-3F3Dokumen22 halamanPerancangan Sistem Informasi Logistik Dan Basis Data: ILI-3F3PRAFAJAR SUKSESSANNO MUTTAQINBelum ada peringkat
- Staffing: Why Is Staffing Essential?Dokumen2 halamanStaffing: Why Is Staffing Essential?ARISBelum ada peringkat
- Supply Chain 101 - SAPDokumen34 halamanSupply Chain 101 - SAPuddinn9Belum ada peringkat