Anda mungkin juga menyukai
- Amru 4L - MandarinDokumen2 halamanAmru 4L - MandarinGea Pandhita SBelum ada peringkat
- Amru 4L - ArtDokumen1 halamanAmru 4L - ArtGea Pandhita SBelum ada peringkat
- 2020 01 23 20018549v1 Full PDFDokumen11 halaman2020 01 23 20018549v1 Full PDFLino SabadoBelum ada peringkat
- Screening Cognitive Decline in Dementia: Preliminary Data On The Italian Version of The IQCODE - SPRDokumen2 halamanScreening Cognitive Decline in Dementia: Preliminary Data On The Italian Version of The IQCODE - SPRGea Pandhita SBelum ada peringkat
- The Clock Drawing Test As A Screening Tool in Mild Cognitive Impairment and Very Mild Dementia: A NeDokumen13 halamanThe Clock Drawing Test As A Screening Tool in Mild Cognitive Impairment and Very Mild Dementia: A NeGea Pandhita SBelum ada peringkat
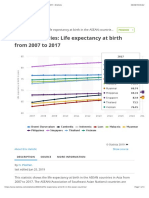
- ASEAN Countries - 1 Life Expectancy at Birth 2007-2017 - StatistaDokumen3 halamanASEAN Countries - 1 Life Expectancy at Birth 2007-2017 - StatistaGea Pandhita SBelum ada peringkat
- CK STUDENT Registration-InstructionsDokumen3 halamanCK STUDENT Registration-InstructionsGea Pandhita SBelum ada peringkat
- Mild Head Injury For KidsDokumen6 halamanMild Head Injury For KidsGea Pandhita SBelum ada peringkat
- The Role of The Montreal Cognitive Assessment (MoCA) and Its Memory Tasks For Detecting Mild CognitiDokumen11 halamanThe Role of The Montreal Cognitive Assessment (MoCA) and Its Memory Tasks For Detecting Mild CognitiGea Pandhita SBelum ada peringkat
- Tugas Telaan Kritis Artikel Penelitian - Intra Arterial Heparin Flushing Increases Manual Muscle Test Medical Research Councils - Gea Pandhita SDokumen6 halamanTugas Telaan Kritis Artikel Penelitian - Intra Arterial Heparin Flushing Increases Manual Muscle Test Medical Research Councils - Gea Pandhita SGea Pandhita SBelum ada peringkat
- Tugas Telaan Kritis Artikel Penelitian - Intra Arterial Heparin Flushing Increases Manual Muscle Test Medical Research Councils - Gea Pandhita SDokumen6 halamanTugas Telaan Kritis Artikel Penelitian - Intra Arterial Heparin Flushing Increases Manual Muscle Test Medical Research Councils - Gea Pandhita SGea Pandhita SBelum ada peringkat
- Medcht00103 0225Dokumen10 halamanMedcht00103 0225Gea Pandhita SBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 12 Core FunctionsDokumen106 halaman12 Core FunctionsEmilyBelum ada peringkat
- Brand Analysis of Leading Sanitary Napkin BrandsDokumen21 halamanBrand Analysis of Leading Sanitary Napkin BrandsSoumya PattnaikBelum ada peringkat
- Pencak Silat Talent ScoutDokumen9 halamanPencak Silat Talent ScoutWisnu Bayu MurtiBelum ada peringkat
- Sdera Demo Lesson DVD Worksheet 2021Dokumen2 halamanSdera Demo Lesson DVD Worksheet 2021api-396577001Belum ada peringkat
- Radiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseDokumen8 halamanRadiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseputriwilujengBelum ada peringkat
- The Digestive System ExplainedDokumen33 halamanThe Digestive System ExplainedGulAwezBelum ada peringkat
- MBSR Standards of Practice 2014Dokumen24 halamanMBSR Standards of Practice 2014wasdunichtsagst100% (1)
- Lung Cancer - Symptoms and Causes - Mayo ClinicDokumen9 halamanLung Cancer - Symptoms and Causes - Mayo ClinicTakuranashe DebweBelum ada peringkat
- Gurr2011-Probleme Psihologice Dupa Atac CerebralDokumen9 halamanGurr2011-Probleme Psihologice Dupa Atac CerebralPaulBelum ada peringkat
- Surgery Final NotesDokumen81 halamanSurgery Final NotesDETECTIVE CONANBelum ada peringkat
- UK Code of Practice For Tampon Manufactures and DistributorsDokumen9 halamanUK Code of Practice For Tampon Manufactures and DistributorsFuzzy_Wood_PersonBelum ada peringkat
- Ijspt 10 734 PDFDokumen14 halamanIjspt 10 734 PDFasmaBelum ada peringkat
- Transmission Substation Work Practice Manual 2016-07-22Dokumen499 halamanTransmission Substation Work Practice Manual 2016-07-22Edmund YoongBelum ada peringkat
- Dr. Nilofer's Guide to Activator & Bionator AppliancesDokumen132 halamanDr. Nilofer's Guide to Activator & Bionator Appliancesdr_nilofervevai2360100% (3)
- Stressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDokumen22 halamanStressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDarleen Rizel CalumbaBelum ada peringkat
- Calculate The Max Doses of Local Anesthesia in DentistryDokumen13 halamanCalculate The Max Doses of Local Anesthesia in DentistryYasser MagramiBelum ada peringkat
- Repair of Obstetric Perineal LacerationsDokumen7 halamanRepair of Obstetric Perineal LacerationsadriantiariBelum ada peringkat
- A Harmonious Smile: Biological CostsDokumen12 halamanA Harmonious Smile: Biological Costsjsjs kaknsbsBelum ada peringkat
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDokumen2 halamanAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoBelum ada peringkat
- Influence of Social Capital On HealthDokumen11 halamanInfluence of Social Capital On HealthHobi's Important BusinesseuBelum ada peringkat
- Ecological PyramidsDokumen19 halamanEcological Pyramidsnandhinidish100% (1)
- Diagram Alir Dan Deskripsi Proses: Tugas 4Dokumen11 halamanDiagram Alir Dan Deskripsi Proses: Tugas 4FevitaBelum ada peringkat
- PancreatoblastomaDokumen16 halamanPancreatoblastomaDr Farman AliBelum ada peringkat
- Soft Drinks in India: Euromonitor International February 2022Dokumen27 halamanSoft Drinks in India: Euromonitor International February 2022Gayathri22394Belum ada peringkat
- UserGuide2015 PDFDokumen114 halamanUserGuide2015 PDFYihan WangBelum ada peringkat
- OCPD: Symptoms, Diagnosis and TreatmentDokumen4 halamanOCPD: Symptoms, Diagnosis and TreatmentRana Muhammad Ahmad Khan ManjBelum ada peringkat
- L Sit ProgramDokumen23 halamanL Sit Programdebo100% (1)
- Tack Welding PowerPointDokumen94 halamanTack Welding PowerPointCheerag100% (1)
- Isolation and Identification of Bacteria ThesisDokumen7 halamanIsolation and Identification of Bacteria Thesisafbtbegxe100% (2)
- Qatar Healthcare Facilities Contact GuideDokumen3 halamanQatar Healthcare Facilities Contact GuideShibu KavullathilBelum ada peringkat