Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Deskripsi LukaDokumen1 halamanDeskripsi Lukaretno widyastutiBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Diabet 1Dokumen9 halamanDiabet 1LauraBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Latihan VERDokumen2 halamanLatihan VERretno widyastutiBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Birth Defects Surveillance A Manual For Programme Managers 2020manual PDokumen248 halamanBirth Defects Surveillance A Manual For Programme Managers 2020manual Pretno widyastutiBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Site Accessibility Contact Mychild Sitemap Select Language Create AccountDokumen42 halamanSite Accessibility Contact Mychild Sitemap Select Language Create Accountretno widyastutiBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Trigger Finger TranslateDokumen11 halamanTrigger Finger Translateretno widyastutiBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Guideline For WorkshopDokumen9 halamanGuideline For Workshopretno widyastutiBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Plastic Surgery ConferenceDokumen1 halamanPlastic Surgery Conferenceretno widyastutiBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Doctors Gonna BeDokumen9 halamanDoctors Gonna Beretno widyastutiBelum ada peringkat
- Neurogenic Bladder Dysfunction: Causes and ManagementDokumen21 halamanNeurogenic Bladder Dysfunction: Causes and Managementretno widyastutiBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Multiple Brain Abscess: A Review of Fourteen Cases.: Author InformationDokumen1 halamanMultiple Brain Abscess: A Review of Fourteen Cases.: Author Informationretno widyastutiBelum ada peringkat
- Peserta TDK 2013Dokumen3 halamanPeserta TDK 2013Galih NugrahaBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Site Accessibility Contact Mychild Sitemap Select Language Create AccountDokumen42 halamanSite Accessibility Contact Mychild Sitemap Select Language Create Accountretno widyastutiBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Effects of Child Sexual AbuseDokumen2 halamanThe Effects of Child Sexual Abuseretno widyastutiBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Skenario B Blok 21Dokumen12 halamanSkenario B Blok 21retno widyastutiBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- DD GoutDokumen2 halamanDD Goutretno widyastutiBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- -Dokumen7 halaman-retno widyastutiBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Peserta TDK 2013Dokumen3 halamanPeserta TDK 2013Galih NugrahaBelum ada peringkat
- Is 10-10-10 Really a Lucky NumberDokumen5 halamanIs 10-10-10 Really a Lucky Numberretno widyastutiBelum ada peringkat
- Katy - Case StudyDokumen27 halamanKaty - Case Studyapi-27696154267% (3)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Healthier: CommunitiesDokumen4 halamanHealthier: CommunitiesymcawncBelum ada peringkat
- Healthy Heart BrochureDokumen2 halamanHealthy Heart BrochureSanjay Somoo100% (1)
- Analysis of The Body Composition of Pole Dance WomenDokumen5 halamanAnalysis of The Body Composition of Pole Dance WomenKatiele TomlinsonBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Eat This Not That GuideDokumen14 halamanEat This Not That Guidexdownloader50% (2)
- 2015 Bull Mock CAT - 09 Ice Cream Sales AnalysisDokumen54 halaman2015 Bull Mock CAT - 09 Ice Cream Sales Analysisyajur_nagiBelum ada peringkat
- Huron Hometown News - July 26, 2012Dokumen8 halamanHuron Hometown News - July 26, 2012schaffnerpubBelum ada peringkat
- Doshas & AgniDokumen9 halamanDoshas & AgniDarshAna PaulaBelum ada peringkat
- Depression and Diabetes Slides ENGDokumen20 halamanDepression and Diabetes Slides ENGMaria Magdalena Dumitru100% (1)
- Metformin - More Than Gold Standard' in The Treatment of Type 2 Diabetes MellitusDokumen10 halamanMetformin - More Than Gold Standard' in The Treatment of Type 2 Diabetes MellitusArga Krittas MaranBelum ada peringkat
- The Importance of Non-Exercise Movement For Longevity: by Dr. MercolaDokumen4 halamanThe Importance of Non-Exercise Movement For Longevity: by Dr. MercolaSellappan MuthusamyBelum ada peringkat
- Diabetes Mellitus With Hypertension (A Case Analysis)Dokumen8 halamanDiabetes Mellitus With Hypertension (A Case Analysis)Phoespha MayangsarieBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Adult Body Mass Index Bmi ChartDokumen2 halamanAdult Body Mass Index Bmi ChartMyo Kyaw KyawBelum ada peringkat
- Review Jurnal International Mengenai DiabetesDokumen2 halamanReview Jurnal International Mengenai DiabetesRhindy Nurnaningsy SBelum ada peringkat
- Ace Final ResultsDokumen15 halamanAce Final ResultsRo ManBelum ada peringkat
- Metformin Ameliorates Diabetes With Metabolic Syndrome Induced Changes in Experimental RatsDokumen11 halamanMetformin Ameliorates Diabetes With Metabolic Syndrome Induced Changes in Experimental RatsGuadalupe Hernandez EquihuaBelum ada peringkat
- Wellness Basics: Nutrition, Health and Wellness.Dokumen32 halamanWellness Basics: Nutrition, Health and Wellness.anon_255024900100% (1)
- Employee ID Badge and Medical Checkup RecordsDokumen7 halamanEmployee ID Badge and Medical Checkup RecordsWellness AMNTBelum ada peringkat
- Sphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeDokumen12 halamanSphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeUzac BenuBelum ada peringkat
- Comparative analysis of contents in popular cold drink brandsDokumen15 halamanComparative analysis of contents in popular cold drink brandsonamdhingraBelum ada peringkat
- Icd 10Dokumen78 halamanIcd 10KumarBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
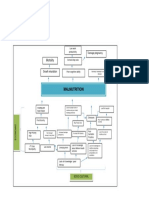
- Problem Tree Analysis MalnutritionDokumen1 halamanProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Essay-Vegan Vs OmnivorousDokumen3 halamanEssay-Vegan Vs OmnivorousStiven Diaz Florez100% (1)
- Unmet Needs in Hispanic/Latino Patients With Type 2 Diabetes MellitusDokumen8 halamanUnmet Needs in Hispanic/Latino Patients With Type 2 Diabetes MellitusChris WilliamsBelum ada peringkat
- 12 Week Bikini Bombshell Workout Plan PDFDokumen9 halaman12 Week Bikini Bombshell Workout Plan PDFGHOST191491100% (1)
- GZCL MethodDokumen11 halamanGZCL MethodRicardo Esteves100% (1)
- Mc. Donalds DownfallDokumen37 halamanMc. Donalds DownfallDhananjay KumarBelum ada peringkat
- Aerobic respiration summaryDokumen30 halamanAerobic respiration summaryadnan muridi100% (1)
- The Food Pyramid GuideDokumen5 halamanThe Food Pyramid GuideSamantha Dayne FernandezBelum ada peringkat
- Nutritional Requirements of GrouperDokumen8 halamanNutritional Requirements of GrouperHafez MabroukBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 5 dari 5 bintang5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)