Anda mungkin juga menyukai
- Social Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsDokumen5 halamanSocial Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsVivian DiazBelum ada peringkat
- What Is Criminology?Dokumen69 halamanWhat Is Criminology?Mir JalalBelum ada peringkat
- Untitled DocumentDokumen12 halamanUntitled DocumentKritika GuptaBelum ada peringkat
- Lanier Epidemiological Criminology DefinitionDokumen41 halamanLanier Epidemiological Criminology DefinitionasesinotufantasmaBelum ada peringkat
- Social Justice: Theories, Issues, and Movements (Revised and Expanded Edition)Dari EverandSocial Justice: Theories, Issues, and Movements (Revised and Expanded Edition)Belum ada peringkat
- Anthropological Perspectives on Public HealthDokumen6 halamanAnthropological Perspectives on Public HealthsugamilasBelum ada peringkat
- The Anthropology of Public HealthDokumen5 halamanThe Anthropology of Public Healthransanaalwis13Belum ada peringkat
- Role of Criminology On The Global Stage 2Dokumen21 halamanRole of Criminology On The Global Stage 2LVT Serrano, Rachel Jane L.Belum ada peringkat
- 1 Toward Unified Criminology Robert Agnew PDFDokumen9 halaman1 Toward Unified Criminology Robert Agnew PDFMiguel VelázquezBelum ada peringkat
- Brownson - Applied Epidemiology - Theory To Practice PDFDokumen413 halamanBrownson - Applied Epidemiology - Theory To Practice PDFGentic Nguyen100% (3)
- Topic 1: Introduction, Scope and Significance of CriminologyDokumen4 halamanTopic 1: Introduction, Scope and Significance of CriminologyNasir HussainBelum ada peringkat
- Social Causation and Social ConstructionDokumen6 halamanSocial Causation and Social Constructionhuberpadilla100% (1)
- Social Epidemiology-Oxford University Press 2014Dokumen641 halamanSocial Epidemiology-Oxford University Press 2014Katherine Kath75% (4)
- 1 Link and Phelan 1995 Fundamental Cause TheoryDokumen16 halaman1 Link and Phelan 1995 Fundamental Cause TheoryAsif IqbalBelum ada peringkat
- Trostle y Sommerfeld-Medical Anthropology EpidemiologyDokumen23 halamanTrostle y Sommerfeld-Medical Anthropology EpidemiologyMantleBelum ada peringkat
- 1 Medical Sociology LectureDokumen36 halaman1 Medical Sociology LectureBrain RunnerBelum ada peringkat
- Full Text What Is Wrong With EpidemiologyDokumen12 halamanFull Text What Is Wrong With EpidemiologyVictor AnguianoBelum ada peringkat
- Int. J. Epidemiol.-2001-Macdonald-46-7Dokumen8 halamanInt. J. Epidemiol.-2001-Macdonald-46-7K MacdonaldBelum ada peringkat
- Theories and Causes of CrimeDokumen104 halamanTheories and Causes of CrimeKristine Jovinal CasicaBelum ada peringkat
- Social Construction of Illness: Key Insights and Policy ImplicationsDokumen14 halamanSocial Construction of Illness: Key Insights and Policy ImplicationsmymagicookieBelum ada peringkat
- Troubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyDari EverandTroubled Bodies: Critical Perspectives on Postmodernism, Medical Ethics, and the BodyBelum ada peringkat
- Criminology - Module 1Dokumen4 halamanCriminology - Module 1reallyprajwalBelum ada peringkat
- 30.08.22 - All Medicine Is SocialDokumen4 halaman30.08.22 - All Medicine Is SocialPola PhotographyBelum ada peringkat
- Introduction To Public Health - FrenkDokumen198 halamanIntroduction To Public Health - FrenkHector CarrascoBelum ada peringkat
- Criminology NoteDokumen58 halamanCriminology Notesher afganBelum ada peringkat
- Crim 1Dokumen43 halamanCrim 1Charles Notarte RanaraBelum ada peringkat
- Krieger-2014 GotTheoryOnThe21stDokumen12 halamanKrieger-2014 GotTheoryOnThe21stRhabaty JaramilloBelum ada peringkat
- Lezione 2 Soc Suf IngleseDokumen5 halamanLezione 2 Soc Suf IngleseantonioBelum ada peringkat
- The Problem of Evidence-Based MedicineDokumen11 halamanThe Problem of Evidence-Based MedicineCynthia Semá BaltazarBelum ada peringkat
- Exploring New Horizons: Medical Anthropology in Public HealthDokumen6 halamanExploring New Horizons: Medical Anthropology in Public Healthibnu cahyonoBelum ada peringkat
- Project 2Dokumen16 halamanProject 2api-254088268Belum ada peringkat
- AHS 547B (Unit4) Sakshi Garg MSC 4thDokumen5 halamanAHS 547B (Unit4) Sakshi Garg MSC 4thSakshi GargBelum ada peringkat
- Criminology Module Description Module ObjectivesDokumen117 halamanCriminology Module Description Module ObjectivesBarrack koderaBelum ada peringkat
- The Psychology of Criminal Minds: A Comprehensive Guide to Understanding CriminologyDari EverandThe Psychology of Criminal Minds: A Comprehensive Guide to Understanding CriminologyBelum ada peringkat
- Module in Intro To CrimDokumen19 halamanModule in Intro To CrimAngelica Flor S. SimbulBelum ada peringkat
- Narrative Medicine in Education, Practice, and InterventionsDari EverandNarrative Medicine in Education, Practice, and InterventionsBelum ada peringkat
- What to Do about AIDS: Physicians and Mental Health Professionals Discuss the IssuesDari EverandWhat to Do about AIDS: Physicians and Mental Health Professionals Discuss the IssuesBelum ada peringkat
- Institute of Criminal Justice Education Bachelor of Science in CriminologyDokumen9 halamanInstitute of Criminal Justice Education Bachelor of Science in CriminologyDominique Vanessa CatbaganBelum ada peringkat
- Criminology CA #1Dokumen7 halamanCriminology CA #1crystalross2512Belum ada peringkat
- Classical SchoolDokumen9 halamanClassical SchoolJoshua S Mjinja100% (1)
- Radical Health_AbstractsDokumen16 halamanRadical Health_AbstractsFabianeVinenteBelum ada peringkat
- Sociology - Ii Project WorkDokumen25 halamanSociology - Ii Project WorkBhuvaneswari Ram MotupalliBelum ada peringkat
- Notes On Criminology: Scope and Development of CriminologyDokumen15 halamanNotes On Criminology: Scope and Development of CriminologySakinah SakinahBelum ada peringkat
- During The Twentieth CenturyDokumen3 halamanDuring The Twentieth CenturyHimanshu SagarBelum ada peringkat
- NOTES ON CRIMINOLOGICAL RESEARCH Page 35Dokumen27 halamanNOTES ON CRIMINOLOGICAL RESEARCH Page 35Joseph Vincent A Salvador100% (1)
- Lecture 42: New Issues Before The Sociologists Slide 1Dokumen18 halamanLecture 42: New Issues Before The Sociologists Slide 1Jaf ShahBelum ada peringkat
- The Biomedical Standardization of Premenstrual SyndromeDokumen15 halamanThe Biomedical Standardization of Premenstrual Syndromelucre88Belum ada peringkat
- Patients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine, and PsychiatryDari EverandPatients and Healers in the Context of Culture: An Exploration of the Borderland between Anthropology, Medicine, and PsychiatryPenilaian: 4 dari 5 bintang4/5 (4)
- Risky Bodies, Drugs and Biopolitics - On The Pharmaceutical Governance of Addiction and Other Diseases of Risk.'Dokumen23 halamanRisky Bodies, Drugs and Biopolitics - On The Pharmaceutical Governance of Addiction and Other Diseases of Risk.'Charlotte AgliataBelum ada peringkat
- Chapter9 EpiMethodsDokumen19 halamanChapter9 EpiMethodsStella NenkeulaBelum ada peringkat
- EPIDEMIOLOGY - BevDokumen55 halamanEPIDEMIOLOGY - BevPINAO-AN, ZANNIELLE GEA L.Belum ada peringkat
- Descartes and the Post-Traumatic Subject: Zizek on the New WoundedDokumen14 halamanDescartes and the Post-Traumatic Subject: Zizek on the New WoundedasesinotufantasmaBelum ada peringkat
- Mujeres Encarceladas MundoDokumen6 halamanMujeres Encarceladas MundoasesinotufantasmaBelum ada peringkat
- Social Perspectives ViollDokumen19 halamanSocial Perspectives ViollasesinotufantasmaBelum ada peringkat
- 397 Akers EpiCrimDokumen6 halaman397 Akers EpiCrimasesinotufantasmaBelum ada peringkat
- (Ninth Edition) : Roy WalmsleyDokumen6 halaman(Ninth Edition) : Roy WalmsleyasesinotufantasmaBelum ada peringkat
- Wood JC 479.fullDokumen20 halamanWood JC 479.fullasesinotufantasmaBelum ada peringkat
- (Ninth Edition) : Roy WalmsleyDokumen6 halaman(Ninth Edition) : Roy WalmsleyasesinotufantasmaBelum ada peringkat
- Social Perspectives ViollDokumen19 halamanSocial Perspectives ViollasesinotufantasmaBelum ada peringkat
- Eisner 473.fullDokumen6 halamanEisner 473.fullasesinotufantasmaBelum ada peringkat
- 397 Akers EpiCrimDokumen6 halaman397 Akers EpiCrimasesinotufantasmaBelum ada peringkat
- 397 Akers EpiCrimDokumen6 halaman397 Akers EpiCrimasesinotufantasmaBelum ada peringkat
- Ending Violence AgainstDokumen32 halamanEnding Violence AgainstasesinotufantasmaBelum ada peringkat
- ScienceDokumen3 halamanScienceKezia SantosidadBelum ada peringkat
- Biography of John VennDokumen2 halamanBiography of John VennReggieBasong100% (1)
- Pragmatism and EducationDokumen21 halamanPragmatism and EducationV.K. Maheshwari91% (74)
- Repetition in Language Teaching and LearningDokumen17 halamanRepetition in Language Teaching and LearningRodrigo López Escobedo100% (1)
- Sosiologi Paper K3Dokumen6 halamanSosiologi Paper K3romadhon fahmiBelum ada peringkat
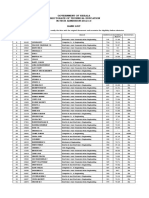
- Government of Kerala Directorate of Technical Education M.TECH ADMISSION 2012-13 Rank ListDokumen126 halamanGovernment of Kerala Directorate of Technical Education M.TECH ADMISSION 2012-13 Rank ListMidhun MuraliBelum ada peringkat
- Tugas Bu Heni Jurnal Ratu Khoirotun Nisa FormatifDokumen21 halamanTugas Bu Heni Jurnal Ratu Khoirotun Nisa FormatifRatu nisaBelum ada peringkat
- The Scientific MethodDokumen22 halamanThe Scientific Methodsohail mohammad (Style de sohail)Belum ada peringkat
- CJR Penyesuaian DiriDokumen11 halamanCJR Penyesuaian DiriRonãl SchweinsteigerBelum ada peringkat
- The Sensist Nominalism of HobbesDokumen38 halamanThe Sensist Nominalism of HobbesPaul HorriganBelum ada peringkat
- Interpersonal RelationshipDokumen62 halamanInterpersonal RelationshipPrabhjot Singh100% (1)
- Advantages and Disadvantages of ObservationDokumen3 halamanAdvantages and Disadvantages of ObservationReymond NicolasBelum ada peringkat
- Quantitative ResearchDokumen131 halamanQuantitative ResearchJest Del RosarioBelum ada peringkat
- Experimental Research MethodsDokumen25 halamanExperimental Research Methodslololo loloBelum ada peringkat
- There S No Testimonial Justice Why Pursuit of A Virtue Is Not The Solution To Epistemic Injustice PDFDokumen23 halamanThere S No Testimonial Justice Why Pursuit of A Virtue Is Not The Solution To Epistemic Injustice PDFana lauraBelum ada peringkat
- Communication Theory and Systems PDFDokumen2 halamanCommunication Theory and Systems PDFJamieBelum ada peringkat
- Theoria Volume 74 Issue 2 2008 (Doi 10.1111 - j.1755-2567.2008.00011.x) JACOB BUSCH - No New Miracles, Same Old TricksDokumen13 halamanTheoria Volume 74 Issue 2 2008 (Doi 10.1111 - j.1755-2567.2008.00011.x) JACOB BUSCH - No New Miracles, Same Old TricksVladDolghiBelum ada peringkat
- Philosophy Notes 2Dokumen4 halamanPhilosophy Notes 2Eleonor AlanoBelum ada peringkat
- The Different PhilosophersDokumen17 halamanThe Different PhilosophersJohanna ArinasBelum ada peringkat
- Educational Theories of Cognitive DevelopmentDokumen10 halamanEducational Theories of Cognitive DevelopmentFoqia AliBelum ada peringkat
- Introduction to Validity, Reliability and Their EstimationDokumen6 halamanIntroduction to Validity, Reliability and Their EstimationWinifridaBelum ada peringkat
- L2 Qualitative ResearchDokumen16 halamanL2 Qualitative ResearchTrishia Aloro100% (4)
- Introduction To Stages of AIDokumen9 halamanIntroduction To Stages of AIMarkapuri Santhoash kumarBelum ada peringkat
- Expanding Research Methods with the Power of BricolageDokumen22 halamanExpanding Research Methods with the Power of BricolageYaimar MontoyaBelum ada peringkat
- Crime RP PDFDokumen20 halamanCrime RP PDFprincess sanaBelum ada peringkat
- 2019 Inductive Versus Deductive Teaching MethodsDokumen21 halaman2019 Inductive Versus Deductive Teaching MethodsAlanFizaDaniBelum ada peringkat
- DevianceDokumen6 halamanDevianceMichael Alan CohenBelum ada peringkat
- CMY3701 Study GuideDokumen207 halamanCMY3701 Study GuideDarrellBelum ada peringkat
- Economic Education ProposalDokumen7 halamanEconomic Education Proposalyuliaarya sastiBelum ada peringkat
- (Michael Byram, Veronica Esarte-Sarries, Susan Tay (BookFi) PDFDokumen439 halaman(Michael Byram, Veronica Esarte-Sarries, Susan Tay (BookFi) PDFPegiawan BasopiBelum ada peringkat