Anda mungkin juga menyukai
- BCRC Dec 2014 ScheduleDokumen16 halamanBCRC Dec 2014 SchedulejmfleckBelum ada peringkat
- 2014-2015 Dance ClassDokumen1 halaman2014-2015 Dance ClassjmfleckBelum ada peringkat
- Jump Stretch November 2014Dokumen2 halamanJump Stretch November 2014jmfleckBelum ada peringkat
- Nov 2014 ScheduleDokumen8 halamanNov 2014 SchedulejmfleckBelum ada peringkat
- Cycling & Hot Yoga Nov 2014 CalendarDokumen1 halamanCycling & Hot Yoga Nov 2014 CalendarjmfleckBelum ada peringkat
- Gymnastics Registration Payment Due 2013-2014Dokumen1 halamanGymnastics Registration Payment Due 2013-2014jmfleckBelum ada peringkat
- Youth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimeDokumen1 halamanYouth Gymnastics Class Schedule 2014-2015: Class Ages DAY TimejmfleckBelum ada peringkat
- Pool ScheduleDokumen1 halamanPool SchedulejmfleckBelum ada peringkat
- Jump Stretch November 2014Dokumen2 halamanJump Stretch November 2014jmfleckBelum ada peringkat
- August 2014 ScheduleDokumen16 halamanAugust 2014 SchedulejmfleckBelum ada peringkat
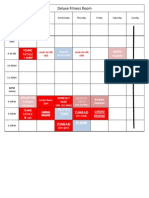
- Deluxe Fitness Nov 2014 CalendarDokumen1 halamanDeluxe Fitness Nov 2014 CalendarjmfleckBelum ada peringkat
- 2014-2015 Dance Class RegistrationDokumen1 halaman2014-2015 Dance Class RegistrationjmfleckBelum ada peringkat
- All Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance ScheduleDokumen1 halamanAll Questions, Contact: Michelle Bower (724) 699-4383: 2014-2015 Dance SchedulejmfleckBelum ada peringkat
- 5K FormDokumen2 halaman5K FormjmfleckBelum ada peringkat
- TriFold - 5KDokumen2 halamanTriFold - 5KjmfleckBelum ada peringkat
- Health HistoryDokumen1 halamanHealth HistoryjmfleckBelum ada peringkat
- Expo 2014 FormDokumen1 halamanExpo 2014 FormjmfleckBelum ada peringkat
- Gymnastics Registration 2014Dokumen1 halamanGymnastics Registration 2014jmfleckBelum ada peringkat
- Deluxe Fitness BrochuresDokumen2 halamanDeluxe Fitness BrochuresjmfleckBelum ada peringkat
- Jump Stretch August 2014Dokumen2 halamanJump Stretch August 2014jmfleckBelum ada peringkat
- Intake FormDokumen1 halamanIntake FormjmfleckBelum ada peringkat
- July 2014 ScheduleDokumen12 halamanJuly 2014 SchedulejmfleckBelum ada peringkat
- J Marcus FleckDokumen1 halamanJ Marcus FleckjmfleckBelum ada peringkat
- 1st Annual Golf Scramble BrochureDokumen2 halaman1st Annual Golf Scramble BrochurejmfleckBelum ada peringkat
- Pre School CampDokumen1 halamanPre School CampjmfleckBelum ada peringkat
- Wish ListDokumen3 halamanWish ListjmfleckBelum ada peringkat
- Racquetball TournamentDokumen1 halamanRacquetball TournamentjmfleckBelum ada peringkat
- Best of The BestDokumen1 halamanBest of The BestjmfleckBelum ada peringkat
- 401 - Northern Route To Downtown Sharon (Monday-Friday)Dokumen9 halaman401 - Northern Route To Downtown Sharon (Monday-Friday)jmfleckBelum ada peringkat
- HistoryDokumen1 halamanHistoryjmfleckBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Managerial Accounting Chapter 5 SolutionsDokumen71 halamanManagerial Accounting Chapter 5 SolutionsSyed Atiq TurabiBelum ada peringkat
- Frequency Asked Questions For: Smartbroadband Wireless PrepaidDokumen5 halamanFrequency Asked Questions For: Smartbroadband Wireless PrepaidBiswajit SikdarBelum ada peringkat
- Case Study Questions Product ManagerDokumen4 halamanCase Study Questions Product ManagerClinton OnyenemezuBelum ada peringkat
- Khmer JobDokumen1 halamanKhmer JobNara VoramanBelum ada peringkat
- Basel Norms - Bane or BoonDokumen7 halamanBasel Norms - Bane or BoonSooraj KumarBelum ada peringkat
- Seatwork 5Dokumen2 halamanSeatwork 5Jasmine ManingoBelum ada peringkat
- Geograohical Infos of Cebu: Step 1Dokumen3 halamanGeograohical Infos of Cebu: Step 1Jessica ArantonBelum ada peringkat
- Credit Card ProcessingDokumen58 halamanCredit Card ProcessingDipanwita Bhuyan92% (13)
- Task 6Dokumen3 halamanTask 6Ansell CristianBelum ada peringkat
- Didi Trip Receipt List: Driver InformationDokumen1 halamanDidi Trip Receipt List: Driver InformationkayyumanwarBelum ada peringkat
- Supply Chain Management: OBS SC-ProcessesDokumen24 halamanSupply Chain Management: OBS SC-ProcessesNaureen AyubBelum ada peringkat
- Completing The Tests in The Acquisition and Payment Cycle: Verification of Selected AccountsDokumen46 halamanCompleting The Tests in The Acquisition and Payment Cycle: Verification of Selected AccountsFadhliatulQisthiBelum ada peringkat
- Promote NMT Usage in VijayawadaDokumen10 halamanPromote NMT Usage in VijayawadaPavani SingamsettyBelum ada peringkat
- Framework For Mobile Money Implementation in NigerDokumen9 halamanFramework For Mobile Money Implementation in Nigernocode pulseBelum ada peringkat
- Viva Edexcel Gcse Ap m3 ListeningDokumen4 halamanViva Edexcel Gcse Ap m3 ListeningJosé Manuel Rodríguez SánchezBelum ada peringkat
- Mutov122164407 01062023-07082023Dokumen7 halamanMutov122164407 01062023-07082023sreekanthBelum ada peringkat
- Working Capital ManagementDokumen78 halamanWorking Capital ManagementDrj Maz50% (2)
- Internship Report On BALDokumen96 halamanInternship Report On BALM I HASSANBelum ada peringkat
- Retrieve DocumentDokumen4 halamanRetrieve DocumentStrahinja AndreasBelum ada peringkat
- Cybercrime in Banking Sector Project for Mumbai UniversityDokumen44 halamanCybercrime in Banking Sector Project for Mumbai UniversityPranav ViraBelum ada peringkat
- 7090-15 CEM Packet Transport PlatformDokumen3 halaman7090-15 CEM Packet Transport PlatformAbbas MaghazehiBelum ada peringkat
- Resultado: Buscar Fabricante o Prefijos MACDokumen10 halamanResultado: Buscar Fabricante o Prefijos MACJosé LuisBelum ada peringkat
- Schedule Yuran Sem 1 Sesi 20202021 MBADokumen1 halamanSchedule Yuran Sem 1 Sesi 20202021 MBAM NaszriBelum ada peringkat
- E BankingDokumen102 halamanE BankingSwati Mann60% (5)
- Consumer Preference for Online Travel PortalsDokumen144 halamanConsumer Preference for Online Travel PortalsVaibhav BahetiBelum ada peringkat
- Insurance ProDokumen39 halamanInsurance ProSyedFaisalHasanShahBelum ada peringkat
- Absolute Best Online Roulette CasinoDokumen10 halamanAbsolute Best Online Roulette CasinoYan MikhlinBelum ada peringkat
- Date Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceDokumen3 halamanDate Narration Chq./Ref - No. Value DT Withdrawal Amt. Deposit Amt. Closing BalanceBikram PaulBelum ada peringkat
- Sales PromotionDokumen10 halamanSales PromotionAdnan patelBelum ada peringkat
- ChallanDokumen1 halamanChallannaresh maddu100% (1)