Anda mungkin juga menyukai
- The New Alkaline Diet To Beat Kidney Disease: Avoid DialysisDari EverandThe New Alkaline Diet To Beat Kidney Disease: Avoid DialysisBelum ada peringkat
- Restoring Your Digestive Health:: A Proven Plan to Conquer Crohn's, Colitis, and Digestive DiseasesDari EverandRestoring Your Digestive Health:: A Proven Plan to Conquer Crohn's, Colitis, and Digestive DiseasesBelum ada peringkat
- Detection Threshold and Sensory Preference For Salty Taste Among Malay, Chinese and Indian Students in Health Campus, Universiti Sains MalaysiaDokumen8 halamanDetection Threshold and Sensory Preference For Salty Taste Among Malay, Chinese and Indian Students in Health Campus, Universiti Sains MalaysiaVAIDEHI ULAGANATHANBelum ada peringkat
- Balan 2013Dokumen7 halamanBalan 2013VAIDEHI ULAGANATHANBelum ada peringkat
- Menstrual Taste BudsDokumen4 halamanMenstrual Taste BudsadiudaBelum ada peringkat
- Treatment HeartburnDokumen2 halamanTreatment HeartburnnurainiBelum ada peringkat
- Multidimensional Evaluation of Endogenous and Health Factors Affecting Food Preferences, Taste and Smell PerceptionDokumen11 halamanMultidimensional Evaluation of Endogenous and Health Factors Affecting Food Preferences, Taste and Smell Perceptiongiuseppe.versari.97Belum ada peringkat
- Jurnal ZulfaDokumen5 halamanJurnal ZulfaCaesar CorleoneBelum ada peringkat
- Salt Reduction Lowers Cardiovascular Risk: Meta-Analysis of Outcome TrialsDokumen3 halamanSalt Reduction Lowers Cardiovascular Risk: Meta-Analysis of Outcome Trialsapi-69964648Belum ada peringkat
- Asupan Makan, Sindrom Metabolik, Dan Status Keseimbangan Asam-Basa Pada LansiaDokumen9 halamanAsupan Makan, Sindrom Metabolik, Dan Status Keseimbangan Asam-Basa Pada LansiaKristinBelum ada peringkat
- Nutrients 12 01449Dokumen8 halamanNutrients 12 01449gelajeon97Belum ada peringkat
- Appetite: John C. Peters, Sarit Polsky, Rebecca Stark, Pan Zhaoxing, James O. HillDokumen6 halamanAppetite: John C. Peters, Sarit Polsky, Rebecca Stark, Pan Zhaoxing, James O. HillMaribel Londoño FlórezBelum ada peringkat
- Estimation of Salivary GlucoseDokumen10 halamanEstimation of Salivary GlucoseSuganya MurugaiahBelum ada peringkat
- The Acid Alkaline Food Guide - Dr. Susan Brown PDFDokumen153 halamanThe Acid Alkaline Food Guide - Dr. Susan Brown PDFepanama100% (1)
- Higher Selenium Status Is Associated With Adverse Blood Lipid Profile in British AdultsDokumen7 halamanHigher Selenium Status Is Associated With Adverse Blood Lipid Profile in British AdultsHerly Maulida SurdhawatiBelum ada peringkat
- The Acid Alkaline FoodDokumen146 halamanThe Acid Alkaline FoodDana Sarah88% (8)
- Pola Konsumsi Natrium Dan Lemak Sebagai Faktor Risiko Terjadinya Penyakit Hipertensi Di Wilayah Kerja Puskesmas Kandangan Kecamatan Kandangan Kabupaten Hulu Sungai SelatanDokumen7 halamanPola Konsumsi Natrium Dan Lemak Sebagai Faktor Risiko Terjadinya Penyakit Hipertensi Di Wilayah Kerja Puskesmas Kandangan Kecamatan Kandangan Kabupaten Hulu Sungai SelatanRaudatus SLechaBelum ada peringkat
- Non-Cephalic Presentation in Late Pregnancy: EditorialsDokumen2 halamanNon-Cephalic Presentation in Late Pregnancy: EditorialsNinosk Mendoza SolisBelum ada peringkat
- Bumil Anemia KekDokumen7 halamanBumil Anemia KekRita WahyuningsihBelum ada peringkat
- Om 5Dokumen3 halamanOm 5Ucc Ang BangarenBelum ada peringkat
- Jurnal 2-2Dokumen7 halamanJurnal 2-2Surya Andri AntaraBelum ada peringkat
- 3.5 Impact of Proposal On The Pursuit of HappinessDokumen3 halaman3.5 Impact of Proposal On The Pursuit of Happinessrjay manaloBelum ada peringkat
- Title of The StudyDokumen4 halamanTitle of The StudyStafan AlexBelum ada peringkat
- Related StudiesDokumen4 halamanRelated StudiesJohanine VillasantiagoBelum ada peringkat
- Oral Zinc For Treating Diarrhoea in Children: Marzia Lazzerini, Luca RonfaniDokumen2 halamanOral Zinc For Treating Diarrhoea in Children: Marzia Lazzerini, Luca RonfaniCristhian RodriguezBelum ada peringkat
- Breakfast SkippingDokumen6 halamanBreakfast SkippingselviannisameldiBelum ada peringkat
- Slow EatingDokumen10 halamanSlow Eatingapi-240611862Belum ada peringkat
- Chan 2009Dokumen12 halamanChan 2009veaceslav coscodanBelum ada peringkat
- Changes To The General Nutrition QuestionnaireDokumen3 halamanChanges To The General Nutrition QuestionnaireBushra KainaatBelum ada peringkat
- Type1 DiabetesDokumen7 halamanType1 DiabetesbettyborbleBelum ada peringkat
- Draft 1Dokumen8 halamanDraft 1api-286662071Belum ada peringkat
- Shepherd 1984Dokumen11 halamanShepherd 1984VAIDEHI ULAGANATHANBelum ada peringkat
- Comparison of The Atkins Ornish Weight Watchers and Zone Diets For Weight Loss and Heart Disease Risk ReductionDokumen12 halamanComparison of The Atkins Ornish Weight Watchers and Zone Diets For Weight Loss and Heart Disease Risk ReductionbhelelihleBelum ada peringkat
- tmp6D1F TMPDokumen8 halamantmp6D1F TMPFrontiersBelum ada peringkat
- ILSI SEAR Monograph CarbohydratesDokumen108 halamanILSI SEAR Monograph CarbohydratesSemira KarijaševićBelum ada peringkat
- Acido Folico ImpDokumen3 halamanAcido Folico ImpJenny SánchezBelum ada peringkat
- Faecal Microbial Flora and Disease Activity in Rheumatoid Arthritis During A Vegan DietDokumen5 halamanFaecal Microbial Flora and Disease Activity in Rheumatoid Arthritis During A Vegan DietHendra SudaryonoBelum ada peringkat
- LowcarbdietinwomanDokumen8 halamanLowcarbdietinwomanJoão DinizBelum ada peringkat
- Tugas 4Dokumen7 halamanTugas 4faris naufalBelum ada peringkat
- Carbo News 2006Dokumen4 halamanCarbo News 2006s.sabapathyBelum ada peringkat
- 1 SM PDFDokumen7 halaman1 SM PDFsabilaBelum ada peringkat
- Dietary Saturated Fats and Their Food Sources in Relation To The RiskDokumen8 halamanDietary Saturated Fats and Their Food Sources in Relation To The RiskJohn SammutBelum ada peringkat
- 2017 - jfnr-5-9-8 - Plain WaterDokumen5 halaman2017 - jfnr-5-9-8 - Plain WaterdvckpjuBelum ada peringkat
- Dietary Intake DMDokumen9 halamanDietary Intake DMQia BummBelum ada peringkat
- Fast Food, Race/ethnicity, and Income:: A Geographic AnalysisDokumen15 halamanFast Food, Race/ethnicity, and Income:: A Geographic AnalysisGulfishan MirzaBelum ada peringkat
- Effect of Supplementation of Wheat Germ, Bran and GrassDokumen100 halamanEffect of Supplementation of Wheat Germ, Bran and GrassKeval ShethBelum ada peringkat
- Lifestyle Behaviors and Physician Advice For Change Among Overweight and Obese Adults With Prediabetes and Diabetes in The United States, 2006Dokumen9 halamanLifestyle Behaviors and Physician Advice For Change Among Overweight and Obese Adults With Prediabetes and Diabetes in The United States, 2006Agil SulistyonoBelum ada peringkat
- Emerging ScienceDokumen3 halamanEmerging SciencePatty LinBelum ada peringkat
- Hubungan Antara Pola Makan Dengan Kadar Asam Urat Darah Pada Wanita Postmenopause Di Posyandu Lansia Wilayah Kerja Puskesmas DR Soetomo SurabayaDokumen7 halamanHubungan Antara Pola Makan Dengan Kadar Asam Urat Darah Pada Wanita Postmenopause Di Posyandu Lansia Wilayah Kerja Puskesmas DR Soetomo SurabayaAlfinda Diah AjengBelum ada peringkat
- Article of ValidityDokumen6 halamanArticle of Validityyeeting07Belum ada peringkat
- Pilichiewicz 2009Dokumen6 halamanPilichiewicz 2009Stella KwanBelum ada peringkat
- Is Dietary Quality Associated With Depression An Analysis of The Australian Longitudinal Study of Womens Health DataDokumen8 halamanIs Dietary Quality Associated With Depression An Analysis of The Australian Longitudinal Study of Womens Health Dataridha nurrahmadaniBelum ada peringkat
- Therapeutic Effects of Oral Zinc Supplementation On Acute Watery Diarrhea With Moderate Dehydration: A Double-Blind Randomized Clinical TrialDokumen7 halamanTherapeutic Effects of Oral Zinc Supplementation On Acute Watery Diarrhea With Moderate Dehydration: A Double-Blind Randomized Clinical TrialRizqulloh Taufiqul Hakim BarsahBelum ada peringkat
- Dietary Patterns and Colon Cancer Risk in Whites and African Americans in The North Carolina Colon Cancer StudyDokumen8 halamanDietary Patterns and Colon Cancer Risk in Whites and African Americans in The North Carolina Colon Cancer StudyRyneil AlmarioBelum ada peringkat
- Aula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateDokumen15 halamanAula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateRayane SilvaBelum ada peringkat
- Before & After: Living and Eating Well After Weight-Loss SurgeryDari EverandBefore & After: Living and Eating Well After Weight-Loss SurgeryBelum ada peringkat
- The All-New Diabetic Cookbook: A Complete Guide to Easy Meal Preparation and Enjoyable Eating for Healthy LivingDari EverandThe All-New Diabetic Cookbook: A Complete Guide to Easy Meal Preparation and Enjoyable Eating for Healthy LivingBelum ada peringkat
- The Devil in the Garlic: How Sulfur in Your Food Can Cause Anxiety, Hot flashes, IBS, Brain Fog Migraines, Skin Problems, and More, and a Program to Help You Feel Great AgainDari EverandThe Devil in the Garlic: How Sulfur in Your Food Can Cause Anxiety, Hot flashes, IBS, Brain Fog Migraines, Skin Problems, and More, and a Program to Help You Feel Great AgainBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsDari EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsBelum ada peringkat
- The Plant-Powered Diet: The Lifelong Eating Plan for Achieving Optimal Health, Beginning TodayDari EverandThe Plant-Powered Diet: The Lifelong Eating Plan for Achieving Optimal Health, Beginning TodayPenilaian: 4.5 dari 5 bintang4.5/5 (2)
- A Detailed Lesson Plan in Grade 5 Adjectives ObjectivesDokumen7 halamanA Detailed Lesson Plan in Grade 5 Adjectives ObjectivesLovely ParaisoBelum ada peringkat
- Perfect Puppy in 7 Days - Potty TrainingDokumen0 halamanPerfect Puppy in 7 Days - Potty Trainingingrid_morales_10% (1)
- General Science (Biological Sciences) : Dr. Sanawar IqbalDokumen19 halamanGeneral Science (Biological Sciences) : Dr. Sanawar IqbalAbdullah khalidBelum ada peringkat
- HSE-03 - Kitchen Inspection ChecklistDokumen3 halamanHSE-03 - Kitchen Inspection ChecklistMaheshwor Man JoshiBelum ada peringkat
- 1000 English Collocations in 10 Minutes A DayDokumen128 halaman1000 English Collocations in 10 Minutes A DayKaksak VisagieBelum ada peringkat
- Wild Ducks: Richard GilbertDokumen11 halamanWild Ducks: Richard GilbertRichard GilbertBelum ada peringkat
- Quiz On ReadingDokumen4 halamanQuiz On ReadingMilagros Rodriguez (Mili)Belum ada peringkat
- Backyard Aquaponics Magazine 1Dokumen36 halamanBackyard Aquaponics Magazine 1Anonymous zvbJbW5Wg1Belum ada peringkat
- Healthy Youth PRDokumen1 halamanHealthy Youth PRapi-468683480Belum ada peringkat
- 617 - 9 - New Total English Intermediate. SB VideoScriptsDokumen19 halaman617 - 9 - New Total English Intermediate. SB VideoScriptsBruno GarciaBelum ada peringkat
- SwiggyDokumen5 halamanSwiggyAravind NarayanBelum ada peringkat
- Urban Dictionary PizzaDokumen1 halamanUrban Dictionary PizzaLandon SarnoBelum ada peringkat
- Tip Sheet 9 - Foodservice: Allergen ManagementDokumen3 halamanTip Sheet 9 - Foodservice: Allergen ManagementLuis ReisBelum ada peringkat
- 2 PizzaKutirDokumen18 halaman2 PizzaKutirkrishnaparimalreddyBelum ada peringkat
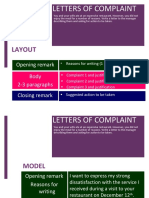
- Letter of ComplaintDokumen12 halamanLetter of ComplaintAscenBelum ada peringkat
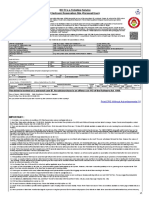
- Train Ticket PDFDokumen2 halamanTrain Ticket PDFVarun Kumar Akula100% (1)
- Knowledge and Rural DevelopmentDokumen84 halamanKnowledge and Rural DevelopmentWilsonRocaBelum ada peringkat
- VIDASA45Dokumen128 halamanVIDASA45thegreatman100% (2)
- Chemistry ProjectDokumen33 halamanChemistry ProjectShubhamBelum ada peringkat
- Bulletin 12 16 11Dokumen3 halamanBulletin 12 16 11Michael AllenBelum ada peringkat
- T-Test For Independent GroupsDokumen14 halamanT-Test For Independent GroupsJM MaguigadBelum ada peringkat
- Cambridge - Science - WB6Dokumen96 halamanCambridge - Science - WB6Long Nguyễn Hoàng90% (10)
- DXN Products South AfricaDokumen15 halamanDXN Products South AfricadxnhpbBelum ada peringkat
- Journal of Food Composition and AnalysisDokumen10 halamanJournal of Food Composition and AnalysisLevin Oval Arroyo OviedoBelum ada peringkat
- Grappa Handbook PDFDokumen66 halamanGrappa Handbook PDFAnonymous ali1kFphBelum ada peringkat
- Breeding Amazons Captivity: Treasure Island. NotDokumen5 halamanBreeding Amazons Captivity: Treasure Island. NotOjeda BorisBelum ada peringkat
- How To Make KapurungDokumen2 halamanHow To Make KapurungNova Claudia Christiani AnggarBelum ada peringkat
- 프렌즈 Season04 ScriptDokumen242 halaman프렌즈 Season04 ScriptbyeoljjiBelum ada peringkat
- Howdy Friends 2Dokumen82 halamanHowdy Friends 2Sori Manasseri100% (2)
- Pop IntroDokumen8 halamanPop IntroSaurabh MundraBelum ada peringkat