Anda mungkin juga menyukai
- Infection Urinary Tract: Escherichia ColiDokumen1 halamanInfection Urinary Tract: Escherichia ColiRaRa PRawitaBelum ada peringkat
- Urolitiasis 2Dokumen1 halamanUrolitiasis 2RaRa PRawitaBelum ada peringkat
- Urinary Tract Infections in Teens and Adults: Topic OverviewDokumen1 halamanUrinary Tract Infections in Teens and Adults: Topic OverviewRaRa PRawitaBelum ada peringkat
- Urolithiasis: Prevalence and IncidenceDokumen3 halamanUrolithiasis: Prevalence and IncidenceRaRa PRawitaBelum ada peringkat
- Toxic Nodular Goiter (TNG) (Or Plummer Syndrome) Is A Condition That Can Occur When A HyperDokumen1 halamanToxic Nodular Goiter (TNG) (Or Plummer Syndrome) Is A Condition That Can Occur When A HyperRaRa PRawitaBelum ada peringkat
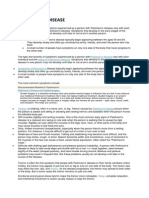
- Parkinson's Disease Stage of Parkinson's DiseaseDokumen2 halamanParkinson's Disease Stage of Parkinson's DiseaseRaRa PRawitaBelum ada peringkat
- Parkinson 2Dokumen1 halamanParkinson 2RaRa PRawitaBelum ada peringkat
- Just To Download File From ScribdDokumen1 halamanJust To Download File From ScribdRaRa PRawitaBelum ada peringkat
- Endogenous Non-Retroviral RNA Virus Elements in Mammalian GenomesDokumen1 halamanEndogenous Non-Retroviral RNA Virus Elements in Mammalian GenomesRaRa PRawitaBelum ada peringkat
- JHGGDokumen1 halamanJHGGRaRa PRawitaBelum ada peringkat
- Just For DownloadDokumen1 halamanJust For DownloadRaRa PRawitaBelum ada peringkat
- Just For DownloadDokumen1 halamanJust For DownloadRaRa PRawitaBelum ada peringkat
- Just To Download File From ScribdDokumen1 halamanJust To Download File From ScribdRaRa PRawitaBelum ada peringkat
- Just To Download File From ScribdDokumen1 halamanJust To Download File From ScribdRaRa PRawitaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Regional Anesthetic Blocks - StatPearls - NCBI BookshelfDokumen7 halamanRegional Anesthetic Blocks - StatPearls - NCBI BookshelfCarolina SidabutarBelum ada peringkat
- Complications and Failure of Airway ManagementDokumen18 halamanComplications and Failure of Airway ManagementNirma RahayuBelum ada peringkat
- Clomifen Citrat PDFDokumen9 halamanClomifen Citrat PDFGilang Andhika SBelum ada peringkat
- Pain Assessment in PediatricDokumen4 halamanPain Assessment in PediatricfitriaBelum ada peringkat
- The Newborn Infant: A Missing Stage in Developmental PsychologyDokumen17 halamanThe Newborn Infant: A Missing Stage in Developmental PsychologyJunia RahmaBelum ada peringkat
- Medicine BOF 2017 OctoberDokumen7 halamanMedicine BOF 2017 Octoberweerawarna fernandoBelum ada peringkat
- ACR 2018 TXIT Exam RationalesDokumen94 halamanACR 2018 TXIT Exam Rationalesgermanfutbol7100% (3)
- Fmge Blue Print PDFDokumen1 halamanFmge Blue Print PDFLesbputih Gelap100% (1)
- Act G ManualDokumen10 halamanAct G ManualMayjie CummosBelum ada peringkat
- Manual of Clinical DieteticsDokumen7 halamanManual of Clinical Dieteticsandi agung0% (1)
- OB Hematologic DiseasesDokumen2 halamanOB Hematologic DiseasespreciousjemBelum ada peringkat
- Chlamydia: Chlamydia Rapid Test Device (Swab/Urine)Dokumen3 halamanChlamydia: Chlamydia Rapid Test Device (Swab/Urine)Cristhian CuviBelum ada peringkat
- Color HandoutsDokumen23 halamanColor HandoutsAndreea SlabuBelum ada peringkat
- Intrapartum Fetal MonitoringDokumen9 halamanIntrapartum Fetal MonitoringYwagar YwagarBelum ada peringkat
- Guideline Newborn Afrika SelatanDokumen102 halamanGuideline Newborn Afrika SelatanM. KurnBelum ada peringkat
- Six Sigma Project WorkDokumen34 halamanSix Sigma Project WorkDrpallavi NanavatiBelum ada peringkat
- Physiological Changes in PregnancyDokumen43 halamanPhysiological Changes in PregnancyDjumadi AkbarBelum ada peringkat
- Pediatric1 PDFDokumen34 halamanPediatric1 PDFNagomi Hanison0% (1)
- Use of Injection Solcoseryl For The Treatment of OligohydramniosDokumen7 halamanUse of Injection Solcoseryl For The Treatment of OligohydramniosJosselle Sempio CalientaBelum ada peringkat
- Birthmarks Identificationandmx201205ryanDokumen4 halamanBirthmarks Identificationandmx201205ryanDanielcc LeeBelum ada peringkat
- Pediatric Neurologic Exam Primitive ReflexesDokumen22 halamanPediatric Neurologic Exam Primitive ReflexesRice CookerBelum ada peringkat
- Procedure ON: Copper-T InsertionDokumen5 halamanProcedure ON: Copper-T Insertionpriyanka100% (2)
- PEDIATRICS Enteral Feeding in NeonatesDokumen3 halamanPEDIATRICS Enteral Feeding in Neonatesnasibdin100% (1)
- Reference List: Benign Prostatic Hyperplasia (BPH)Dokumen17 halamanReference List: Benign Prostatic Hyperplasia (BPH)Naoufel AbbesBelum ada peringkat
- Instrumentar LaparoscopieDokumen3 halamanInstrumentar LaparoscopieMarius NenciuBelum ada peringkat
- 2011 - Policy For Medico Legal Cases (MLC)Dokumen6 halaman2011 - Policy For Medico Legal Cases (MLC)Shawred Analytics100% (1)
- LAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJDokumen24 halamanLAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJIhrom Fatma SaputriBelum ada peringkat
- Hioerplasia Mamaria GestacionalDokumen9 halamanHioerplasia Mamaria GestacionalOctavio LeyvaBelum ada peringkat
- Ethicon Harmonic 300 Ultrasonic Surgery Generator - User ManualDokumen36 halamanEthicon Harmonic 300 Ultrasonic Surgery Generator - User Manualreinahr100% (1)
- The Uses and Limitations of The Fetal Biophysical Profile.Dokumen18 halamanThe Uses and Limitations of The Fetal Biophysical Profile.Diego Ortecho100% (1)