Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Dental Management of Medically Compromised PatientsDokumen12 halamanDental Management of Medically Compromised Patientsمحمد ابوالمجدBelum ada peringkat
- Mil PRF 46010FDokumen20 halamanMil PRF 46010FSantaj Technologies100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Etiology of MalocclusionDokumen28 halamanEtiology of MalocclusionPriyaancaHaarsh100% (3)
- ThiruppavaiDokumen157 halamanThiruppavaiajiva_rts100% (49)
- Biologic Width - The No Encroachment Zone: I J D ADokumen8 halamanBiologic Width - The No Encroachment Zone: I J D AJinny ShawBelum ada peringkat
- Transformers Classics: UK Vol. 3 PreviewDokumen10 halamanTransformers Classics: UK Vol. 3 PreviewGraphic PolicyBelum ada peringkat
- MCQPaperSept 05Dokumen4 halamanMCQPaperSept 05api-26291651100% (1)
- MCQSeptember 2006 Paper IDokumen3 halamanMCQSeptember 2006 Paper Iapi-26291651100% (1)
- Past Tense Irregular Verbs Lesson Plan 02Dokumen7 halamanPast Tense Irregular Verbs Lesson Plan 02drdineshbhmsBelum ada peringkat
- Pratt & Whitney Engine Training ResourcesDokumen5 halamanPratt & Whitney Engine Training ResourcesJulio Abanto50% (2)
- FCC TechDokumen13 halamanFCC TechNguyen Thanh XuanBelum ada peringkat
- Best Practices in Implementing A Secure Microservices ArchitectureDokumen85 halamanBest Practices in Implementing A Secure Microservices Architecturewenapo100% (1)
- Anti Viral DrugsDokumen6 halamanAnti Viral DrugskakuBelum ada peringkat
- PDFDokumen72 halamanPDFGCMediaBelum ada peringkat
- VitaminsDokumen13 halamanVitaminsمحمد ابوالمجدBelum ada peringkat
- Guidelines On Infection Control in Dental ClinicsDokumen10 halamanGuidelines On Infection Control in Dental ClinicsHare RamBelum ada peringkat
- VitaminsDokumen13 halamanVitaminsمحمد ابوالمجدBelum ada peringkat
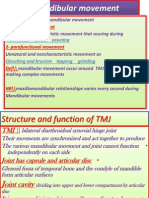
- Mandibular MovementDokumen4 halamanMandibular Movementمحمد ابوالمجدBelum ada peringkat
- Publication PDFDokumen20 halamanPublication PDFمحمد ابوالمجدBelum ada peringkat
- Dental Anatomy DecksDokumen362 halamanDental Anatomy Decksapi-2629165183% (6)
- Anatomy of CNSDokumen32 halamanAnatomy of CNSLeonita AguillonBelum ada peringkat
- Publication PDFDokumen28 halamanPublication PDFمحمد ابوالمجدBelum ada peringkat
- ChemFil Superior44Dokumen27 halamanChemFil Superior44محمد ابوالمجدBelum ada peringkat
- Dental Cements For UseDokumen28 halamanDental Cements For UseAhmed DolaBelum ada peringkat
- Anatomy of CNSDokumen32 halamanAnatomy of CNSLeonita AguillonBelum ada peringkat
- Smear LayerDokumen9 halamanSmear Layerpriyanka_gedamBelum ada peringkat
- Mandibular MovementDokumen4 halamanMandibular Movementمحمد ابوالمجدBelum ada peringkat
- 1Dokumen15 halaman1محمد ابوالمجدBelum ada peringkat
- Emergency MedicineDokumen7 halamanEmergency Medicineمحمد ابوالمجدBelum ada peringkat
- Finishing and PolishingDokumen18 halamanFinishing and Polishingab0maiBelum ada peringkat
- Asnan 7 RulesDokumen2 halamanAsnan 7 Rulesمحمد ابوالمجدBelum ada peringkat
- Anatomy of CNSDokumen32 halamanAnatomy of CNSLeonita AguillonBelum ada peringkat
- OcclusionDokumen17 halamanOcclusionمحمد ابوالمجدBelum ada peringkat
- Behaviour Management 2Dokumen59 halamanBehaviour Management 2Nikhil RaiBelum ada peringkat
- DentistryDokumen71 halamanDentistryAnupama NagrajBelum ada peringkat
- Serial Extraction PedoDokumen23 halamanSerial Extraction PedoSelim BaftiuBelum ada peringkat
- Tooth MovementDokumen14 halamanTooth Movementمحمد ابوالمجدBelum ada peringkat
- RO0111 00-00 WebberDokumen6 halamanRO0111 00-00 WebberARTBelum ada peringkat
- Miles and Snow's Organizational StrategiesDokumen15 halamanMiles and Snow's Organizational StrategiesVirat SahBelum ada peringkat
- Connotative and Denotative, Lexical and StylisticDokumen3 halamanConnotative and Denotative, Lexical and StylisticEman Jay FesalbonBelum ada peringkat
- Talha Farooqi - Assignment 01 - Overview of Bond Sectors and Instruments - Fixed Income Analysis PDFDokumen4 halamanTalha Farooqi - Assignment 01 - Overview of Bond Sectors and Instruments - Fixed Income Analysis PDFMohammad TalhaBelum ada peringkat
- Ice-Cream ConesDokumen6 halamanIce-Cream ConesAlfonso El SabioBelum ada peringkat
- Polyester Staple Fibre Product ListDokumen2 halamanPolyester Staple Fibre Product Listnunu7478Belum ada peringkat
- 6 Economics of International TradeDokumen29 halaman6 Economics of International TradeSenthil Kumar KBelum ada peringkat
- Colorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease LikeDokumen10 halamanColorectal Disease - 2023 - Freund - Can Preoperative CT MR Enterography Preclude The Development of Crohn S Disease Likedavidmarkovic032Belum ada peringkat
- Free ArtistDokumen1 halamanFree Artistnunomgalmeida-1Belum ada peringkat
- Aerospace Propulsion Course Outcomes and Syllabus OverviewDokumen48 halamanAerospace Propulsion Course Outcomes and Syllabus OverviewRukmani Devi100% (2)
- Blood TestsDokumen3 halamanBlood TestsMarycharinelle Antolin MolinaBelum ada peringkat
- Explorations - An Introduction To Astronomy-HighlightsDokumen10 halamanExplorations - An Introduction To Astronomy-HighlightsTricia Rose KnousBelum ada peringkat
- Mock-B1 Writing ReadingDokumen6 halamanMock-B1 Writing ReadingAnonymous 0uBSrduoBelum ada peringkat
- NGOs Affiliated To SWCDokumen2.555 halamanNGOs Affiliated To SWCMandip marasiniBelum ada peringkat
- Year 7 Depth Study 2a 2020 5Dokumen6 halamanYear 7 Depth Study 2a 2020 5api-508928238Belum ada peringkat
- c350 Troubleshooting Guide PDFDokumen94 halamanc350 Troubleshooting Guide PDFPaula Rosal SittlerBelum ada peringkat
- Tahap Kesediaan Pensyarah Terhadap Penggunaan M-Pembelajaran Dalam Sistem Pendidikan Dan Latihan Teknik Dan Vokasional (TVET)Dokumen17 halamanTahap Kesediaan Pensyarah Terhadap Penggunaan M-Pembelajaran Dalam Sistem Pendidikan Dan Latihan Teknik Dan Vokasional (TVET)Khairul Yop AzreenBelum ada peringkat
- UT Dallas Syllabus For Chem2323.001.10s Taught by Sergio Cortes (Scortes)Dokumen9 halamanUT Dallas Syllabus For Chem2323.001.10s Taught by Sergio Cortes (Scortes)UT Dallas Provost's Technology GroupBelum ada peringkat
- MA KP3-V2H-2 enDokumen155 halamanMA KP3-V2H-2 enJavier MiramontesBelum ada peringkat
- Solving Problems Involving Simple Interest: Lesson 2Dokumen27 halamanSolving Problems Involving Simple Interest: Lesson 2Paolo MaquidatoBelum ada peringkat
- Revised Organizational Structure of Railway BoardDokumen4 halamanRevised Organizational Structure of Railway BoardThirunavukkarasu ThirunavukkarasuBelum ada peringkat
- Noise Pollution Control Policy IndiaDokumen10 halamanNoise Pollution Control Policy IndiaAllu GiriBelum ada peringkat