Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- 1.2.7 Cell Membrane Structure and FunctionDokumen5 halaman1.2.7 Cell Membrane Structure and FunctionAYUSH ALTERNATE67% (3)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Suite 1 For Cello Solo For BB (Bass) Clarinet: Johann Sebastian Bach BWV 1007 PréludeDokumen7 halamanSuite 1 For Cello Solo For BB (Bass) Clarinet: Johann Sebastian Bach BWV 1007 Préludewolfgangerl2100% (1)
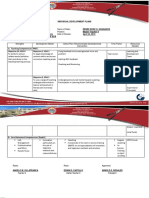
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Dokumen2 halamanIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaBelum ada peringkat
- 2202 Infantilization Essay - Quinn WilsonDokumen11 halaman2202 Infantilization Essay - Quinn Wilsonapi-283151250Belum ada peringkat
- DAA R19 - All UnitsDokumen219 halamanDAA R19 - All Unitspujitha akumallaBelum ada peringkat
- Schedule 1 Allison Manufacturing Sales Budget For The Quarter I Ended March 31 First QuarterDokumen16 halamanSchedule 1 Allison Manufacturing Sales Budget For The Quarter I Ended March 31 First QuarterSultanz Farkhan SukmanaBelum ada peringkat
- WeeblyDokumen6 halamanWeeblyapi-302258377Belum ada peringkat
- Six Sigma PDFDokumen62 halamanSix Sigma PDFssno1Belum ada peringkat
- Corporation Tax CT41G-DciDokumen1 halamanCorporation Tax CT41G-DciHenry HarrodBelum ada peringkat
- Mapua Cwtsstudentsmodule (Ay08 09)Dokumen62 halamanMapua Cwtsstudentsmodule (Ay08 09)anon-805332Belum ada peringkat
- Reading SkillsDokumen8 halamanReading SkillsBob BolBelum ada peringkat
- Windows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwDokumen15 halamanWindows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwYeraldo MarinBelum ada peringkat
- Test 3 - EF Pre-Intermediate - AnswerkeyDokumen3 halamanTest 3 - EF Pre-Intermediate - AnswerkeyMihaela VladuBelum ada peringkat
- KGTE February 2011 ResultDokumen60 halamanKGTE February 2011 ResultSupriya NairBelum ada peringkat
- Sow English Year 4 2023 2024Dokumen12 halamanSow English Year 4 2023 2024Shamien ShaBelum ada peringkat
- Comparative DegreeDokumen25 halamanComparative DegreeAgung PriyanaBelum ada peringkat
- GRP 15 Property Law Final DDokumen15 halamanGRP 15 Property Law Final DBruno OsananBelum ada peringkat
- EY Global Hospitality Insights 2016Dokumen24 halamanEY Global Hospitality Insights 2016Anonymous BkmsKXzwyKBelum ada peringkat
- HG G2 Q1 W57 Module 3 RTPDokumen11 halamanHG G2 Q1 W57 Module 3 RTPJennilyn Amable Democrito100% (1)
- Constantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)Dokumen242 halamanConstantin Floros, Kenneth Chalmers - New Ears For New Music-Peter Lang GMBH, Internationaler Verlag Der Wissenschaften (2014)paperocamillo100% (3)
- Economic and Product Design Considerations in MachiningDokumen29 halamanEconomic and Product Design Considerations in Machininghashir siddiquiBelum ada peringkat
- FOR of Tution Fee: Application ReimbursementDokumen1 halamanFOR of Tution Fee: Application ReimbursementBhavithavBelum ada peringkat
- Narrative ReportDokumen13 halamanNarrative ReportfranceBelum ada peringkat
- Lease of Playground To A SchoolDokumen2 halamanLease of Playground To A SchoolSutapaBelum ada peringkat
- Communique Supply Teacher (Oriental Languages) (Primary) 2021-2022Dokumen4 halamanCommunique Supply Teacher (Oriental Languages) (Primary) 2021-2022nishiBelum ada peringkat
- U.S. Vs Hart, Et Al., 26 Phil 149 CASE DIGESTDokumen2 halamanU.S. Vs Hart, Et Al., 26 Phil 149 CASE DIGESTAaron Ariston100% (2)
- Written Test 4-Book 3Dokumen2 halamanWritten Test 4-Book 3Vinícius MoreiraBelum ada peringkat
- LTE Principle and LTE PlanningDokumen70 halamanLTE Principle and LTE PlanningShain SalimBelum ada peringkat
- ReferencesDokumen12 halamanReferencesBilal RazzaqBelum ada peringkat
- Latihan Soal CausativeDokumen1 halamanLatihan Soal Causativeanakosagista anakosagistaBelum ada peringkat