Anda mungkin juga menyukai
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordDari EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordBelum ada peringkat
- Healthcare Domain QuestionsDokumen5 halamanHealthcare Domain QuestionsNikhil SatavBelum ada peringkat
- Master Patient IndexDokumen6 halamanMaster Patient IndexAhmed YousefBelum ada peringkat
- Analytics Landscape in Healthcare-1Dokumen24 halamanAnalytics Landscape in Healthcare-1positiveworker88Belum ada peringkat
- Medicare Claims Processing Manual: Chapter 12 - Physicians/Nonphysician PractitionersDokumen232 halamanMedicare Claims Processing Manual: Chapter 12 - Physicians/Nonphysician PractitionersAaron RasmussenBelum ada peringkat
- A Him A Code of EthicsDokumen11 halamanA Him A Code of Ethicstccchar100% (3)
- ACHC - Standards - Community RetailDokumen71 halamanACHC - Standards - Community RetailServesh Tiwari100% (2)
- 837P CMS 1500Dokumen8 halaman837P CMS 1500Gajapathi KBelum ada peringkat
- Online Hospital Management SystemDokumen2 halamanOnline Hospital Management Systemyay guruBelum ada peringkat
- The "Epic" Challenge of Optimizing Antimicrobial Stewardship: The Role of Electronic Medical Records and TechnologyDokumen9 halamanThe "Epic" Challenge of Optimizing Antimicrobial Stewardship: The Role of Electronic Medical Records and TechnologyMr XBelum ada peringkat
- Specification of Checklists and Use Cases For AHIMA Information Governance Principles For Health Care (Igphc)Dokumen43 halamanSpecification of Checklists and Use Cases For AHIMA Information Governance Principles For Health Care (Igphc)Kalyan ChinnaBelum ada peringkat
- Ecw EMR Workbook II - Updated - Portage Health PDFDokumen63 halamanEcw EMR Workbook II - Updated - Portage Health PDFSyed Mudussir HusainBelum ada peringkat
- Specification of Use Cases For Information Management Practices in Healthcare: Patient Registration Use CaseDokumen24 halamanSpecification of Use Cases For Information Management Practices in Healthcare: Patient Registration Use Casecooking with shab'sBelum ada peringkat
- 10-04-093 - OBIX 7.x - 8.x Epic Interface Configuration GuideDokumen70 halaman10-04-093 - OBIX 7.x - 8.x Epic Interface Configuration GuideGary Townsend0% (1)
- Project SynopsisDokumen15 halamanProject SynopsisVigneshBelum ada peringkat
- HIS Lesson 4. Health Information SystemsDokumen29 halamanHIS Lesson 4. Health Information SystemsJannela EscomiendoBelum ada peringkat
- Navigating Powerchart For Ed Ob orDokumen2 halamanNavigating Powerchart For Ed Ob orapi-224958119Belum ada peringkat
- ADT DFT ORU: The Most Commonly Used HL7 Message Types IncludeDokumen1 halamanADT DFT ORU: The Most Commonly Used HL7 Message Types IncludeRafi Uddin ShaikBelum ada peringkat
- Medical Coding PPT by Pooji 1Dokumen9 halamanMedical Coding PPT by Pooji 1babupandu925Belum ada peringkat
- EHR StandardsIndia - August 2013-32630521Dokumen54 halamanEHR StandardsIndia - August 2013-32630521kartiksinhBelum ada peringkat
- Ahima Data Quality Management ModelDokumen11 halamanAhima Data Quality Management Modelselinasimpson2301Belum ada peringkat
- Hcpcs Codes LVL 2Dokumen1 halamanHcpcs Codes LVL 2baskarjoBelum ada peringkat
- DICOM Basics - Part 1: Connectivity OverviewDokumen27 halamanDICOM Basics - Part 1: Connectivity OverviewPacientes PruebaBelum ada peringkat
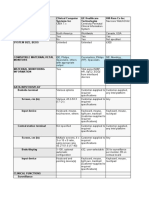
- Clinical Computer Systems ComparisonDokumen12 halamanClinical Computer Systems ComparisonLee ThoongBelum ada peringkat
- EvaluationprogramplanDokumen32 halamanEvaluationprogramplanapi-523878990Belum ada peringkat
- Health Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedDokumen40 halamanHealth Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedsmritiBelum ada peringkat
- 4 Healthmapper Extension ART PDFDokumen38 halaman4 Healthmapper Extension ART PDFTobitusinBelum ada peringkat
- Group 5 - RxnormDokumen26 halamanGroup 5 - RxnormAbdu AminuBelum ada peringkat
- Principles of Healthcare Reimbursement: Sixth EditionDokumen28 halamanPrinciples of Healthcare Reimbursement: Sixth EditionDestiny Hayes100% (2)
- Assg Codingcasestudies 20171109 Ah102 KPDokumen1 halamanAssg Codingcasestudies 20171109 Ah102 KPapi-427618755Belum ada peringkat
- 2021B-Health Information Technology Evaluation Handbook From Meaningful Use To Meaningful OutcomesDokumen199 halaman2021B-Health Information Technology Evaluation Handbook From Meaningful Use To Meaningful Outcomeszeal cocoBelum ada peringkat
- TN ML Manual 2023 - MergedDokumen157 halamanTN ML Manual 2023 - MergedBCBelum ada peringkat
- GEHC-Gateway Project Implementation Guide PDFDokumen30 halamanGEHC-Gateway Project Implementation Guide PDFpreeti dBelum ada peringkat
- Glossary of Billing TermsDokumen8 halamanGlossary of Billing Termscustomerservice.nhaBelum ada peringkat
- IEHP Medi-Cal Members Rights and Responsibilities PDFDokumen11 halamanIEHP Medi-Cal Members Rights and Responsibilities PDFminipower50Belum ada peringkat
- 2) Session 2 - Design and Development of HMISDokumen59 halaman2) Session 2 - Design and Development of HMISyusuf zekeriya mohammedBelum ada peringkat
- Medical Coding SummaryDokumen5 halamanMedical Coding SummaryYhanie De GuzmanBelum ada peringkat
- (AMA) CPT 2021 Professional EditionDokumen3.824 halaman(AMA) CPT 2021 Professional EditionjbmbritoBelum ada peringkat
- HL7Dokumen13 halamanHL7sony100% (3)
- Job Responsibilities of Different Health People PDFDokumen114 halamanJob Responsibilities of Different Health People PDFRuben Paul C RajBelum ada peringkat
- Course OutlineDokumen4 halamanCourse Outlineapi-382689726Belum ada peringkat
- Cdip - 4Dokumen58 halamanCdip - 4SURESHBelum ada peringkat
- BA Healthcare Domain - Interview QuestionsDokumen2 halamanBA Healthcare Domain - Interview QuestionsNikhil Satav100% (1)
- HL7 RimDokumen105 halamanHL7 Rimzmo82Belum ada peringkat
- Barcode Pharmaceutical System Main Project Work Isiyaku AuwaluDokumen30 halamanBarcode Pharmaceutical System Main Project Work Isiyaku Auwalumustapha muhammad AuwalBelum ada peringkat
- Health Information System QuizDokumen5 halamanHealth Information System QuizPhạm Văn Minh0% (1)
- CPT Code Guide - FormattedDokumen29 halamanCPT Code Guide - FormattedAlex KatsnelsonBelum ada peringkat
- Hospital Information Management SystemDokumen13 halamanHospital Information Management SystemSarita yadavBelum ada peringkat
- Design and Implementation of An Online PDokumen14 halamanDesign and Implementation of An Online PRetaj LibyaBelum ada peringkat
- ICL-Coding Operative ReportDokumen33 halamanICL-Coding Operative ReportHIMOfficial100% (2)
- Introduction To Electronic Medical Record - Non-CHKD Employees - August - 2023 V2Dokumen56 halamanIntroduction To Electronic Medical Record - Non-CHKD Employees - August - 2023 V2Ahmad AhmadBelum ada peringkat
- CVS Caremark Q MonthlyDokumen2 halamanCVS Caremark Q MonthlyAngie Henderson MoncadaBelum ada peringkat
- Medical Coding Syllabus EliteDokumen3 halamanMedical Coding Syllabus EliteSujeet KumarBelum ada peringkat
- Master Patient Index FormDokumen2 halamanMaster Patient Index Formapi-355199088Belum ada peringkat
- Breaking Down Barriers to EDCDokumen26 halamanBreaking Down Barriers to EDCin_goodguyBelum ada peringkat
- Xengine Transaction ValidationDokumen12 halamanXengine Transaction ValidationMitchell JohnsonBelum ada peringkat
- Hospital Management System Software in Quanta HisDokumen31 halamanHospital Management System Software in Quanta HisBirlamedisoftBelum ada peringkat
- Hospital information systems overviewDokumen53 halamanHospital information systems overviewkgg1987Belum ada peringkat
- Healthcare Delivery Organization CIOs A Complete Guide - 2019 EditionDari EverandHealthcare Delivery Organization CIOs A Complete Guide - 2019 EditionBelum ada peringkat
- CANNeCTIN 2013.nov.08 Chris Cameron Revised1Dokumen55 halamanCANNeCTIN 2013.nov.08 Chris Cameron Revised1Hanan AhmedBelum ada peringkat
- Presentation ToolsDokumen38 halamanPresentation ToolsHanan AhmedBelum ada peringkat
- French Charts PDFDokumen7 halamanFrench Charts PDFAlina EmBelum ada peringkat
- L'OREAL Social Audit ProgramDokumen24 halamanL'OREAL Social Audit ProgramHanan Ahmed0% (1)
- ASU Eugene SchnellerDokumen11 halamanASU Eugene SchnellerHanan AhmedBelum ada peringkat
- Designing EffectiveDokumen15 halamanDesigning EffectiveHanan AhmedBelum ada peringkat
- Career Options Pharmacy Pharmaceutical SciencesDokumen4 halamanCareer Options Pharmacy Pharmaceutical ScienceszzzamrBelum ada peringkat
- Health Economics and Decision Science (HEDS) School Of Health And Related Research. A comparison of three binary choice methods for health state valuationDokumen25 halamanHealth Economics and Decision Science (HEDS) School Of Health And Related Research. A comparison of three binary choice methods for health state valuationHanan AhmedBelum ada peringkat
- African Newsletter 1 - 2012Dokumen28 halamanAfrican Newsletter 1 - 2012Hanan AhmedBelum ada peringkat
- Cancer AnalystDokumen3 halamanCancer AnalystHanan AhmedBelum ada peringkat
- Future Directions For The Bioinformatics Center: Naomi Altman, Dept. of Statistics Penn StateDokumen32 halamanFuture Directions For The Bioinformatics Center: Naomi Altman, Dept. of Statistics Penn StateHanan AhmedBelum ada peringkat
- Informatics Student BrochureDokumen4 halamanInformatics Student BrochureHanan AhmedBelum ada peringkat
- Building Consensus For The Future Report of The Feasibility Study On Palliative Care For People With DementiaDokumen24 halamanBuilding Consensus For The Future Report of The Feasibility Study On Palliative Care For People With DementiaHanan AhmedBelum ada peringkat
- Hospitals Jenny HargreavesDokumen24 halamanHospitals Jenny HargreavesHanan AhmedBelum ada peringkat
- Indigent Free Pharmacy Feasibilty StudyDokumen6 halamanIndigent Free Pharmacy Feasibilty StudyHanan AhmedBelum ada peringkat
- Egypt's Pharmaceutical Pricing and Reimbursement SystemDokumen6 halamanEgypt's Pharmaceutical Pricing and Reimbursement SystemHanan AhmedBelum ada peringkat
- Managing The Health Care Supply ChainDokumen18 halamanManaging The Health Care Supply ChainHanan AhmedBelum ada peringkat
- Synth-Matrix Ang v2Dokumen6 halamanSynth-Matrix Ang v2Hanan AhmedBelum ada peringkat
- International Seminar on HE and HTA in Egypt: How does HTA support Patient ValueDokumen5 halamanInternational Seminar on HE and HTA in Egypt: How does HTA support Patient ValueHanan AhmedBelum ada peringkat
- Hospitals Jenny HargreavesDokumen24 halamanHospitals Jenny HargreavesHanan AhmedBelum ada peringkat
- Fact Sheet Porto MarinaDokumen2 halamanFact Sheet Porto Marinaaya ahmedBelum ada peringkat
- Mairin Ryan PresentationDokumen29 halamanMairin Ryan PresentationHanan AhmedBelum ada peringkat
- Iqm CMQ OeDokumen1 halamanIqm CMQ OeHanan AhmedBelum ada peringkat
- Brochure Cairo 2013Dokumen9 halamanBrochure Cairo 2013Hanan AhmedBelum ada peringkat
- DR - Ismail HamedDokumen25 halamanDR - Ismail HamedHanan AhmedBelum ada peringkat
- Health Economics For Prescribers: Richard Smith (MED) David Wright (CAP)Dokumen33 halamanHealth Economics For Prescribers: Richard Smith (MED) David Wright (CAP)Hanan AhmedBelum ada peringkat
- The Pharmaceutical Industry: Career Opportunities For PharmacistsDokumen8 halamanThe Pharmaceutical Industry: Career Opportunities For PharmacistsHanan AhmedBelum ada peringkat
- Clinical PharmacyDokumen22 halamanClinical PharmacyHanan AhmedBelum ada peringkat
- SDB Pharmaceutical PresentationDokumen18 halamanSDB Pharmaceutical PresentationHanan Ahmed0% (1)
- Board RMH Pharmacy OLDokumen6 halamanBoard RMH Pharmacy OLHanan AhmedBelum ada peringkat
- AT-8600 Series Switch: Hardware ReferenceDokumen30 halamanAT-8600 Series Switch: Hardware ReferenceSubbuBelum ada peringkat
- Validity Checks: Processing ControlsDokumen3 halamanValidity Checks: Processing Controlsjhela18Belum ada peringkat
- Enterprise, Innovation Creativity 2018-19 S3 CourseworkDokumen7 halamanEnterprise, Innovation Creativity 2018-19 S3 CourseworkSajidBelum ada peringkat
- Company Profile - QuosphereDokumen5 halamanCompany Profile - QuosphereDivya Rao100% (2)
- Selecting Arrester MCOV-UcDokumen9 halamanSelecting Arrester MCOV-Ucjose GonzalezBelum ada peringkat
- Abb CatDokumen9 halamanAbb CatMukesh Kumar MeenaBelum ada peringkat
- Konica 7020 Error Codes: Code DescriptionDokumen3 halamanKonica 7020 Error Codes: Code Descriptionsaito36Belum ada peringkat
- FrlsDokumen25 halamanFrlssudeepjosephBelum ada peringkat
- True/False: List of Attempted Questions and AnswersDokumen15 halamanTrue/False: List of Attempted Questions and AnswersDeepak Kumar VermaBelum ada peringkat
- Spec - LA 11,22,33 KV LA R1 Sep10Dokumen14 halamanSpec - LA 11,22,33 KV LA R1 Sep10Amarjit KulkarniBelum ada peringkat
- L-990 Sensor Tap: Codes Power Supply Temperature Control WeightDokumen3 halamanL-990 Sensor Tap: Codes Power Supply Temperature Control WeightNguyên Trịnh CaoBelum ada peringkat
- Cie - Publist - 2008 Penerangan PDFDokumen11 halamanCie - Publist - 2008 Penerangan PDFAli RosidiBelum ada peringkat
- MS Gree Aircon Midwall Service Manual PDFDokumen55 halamanMS Gree Aircon Midwall Service Manual PDFMacSparesBelum ada peringkat
- CADAM 2000 - Model ParametersDokumen3 halamanCADAM 2000 - Model ParametersAqua MaBelum ada peringkat
- Palm Tower 3 Coverage ReportDokumen61 halamanPalm Tower 3 Coverage ReportHassan DaudBelum ada peringkat
- Director Insurance Development Optimization in Cleveland OH Resume Samuel BeldenDokumen3 halamanDirector Insurance Development Optimization in Cleveland OH Resume Samuel BeldenSamuelBeldenBelum ada peringkat
- Plexus 2 DocumentationDokumen29 halamanPlexus 2 DocumentationHeberto MonroyBelum ada peringkat
- Atmos GIGA N 32-160Dokumen1 halamanAtmos GIGA N 32-160Efril dilen franciscoBelum ada peringkat
- DesuperheatersDokumen8 halamanDesuperheatersmuhdrijasmBelum ada peringkat
- Environmental Management Plan - MatrixDokumen6 halamanEnvironmental Management Plan - Matrixplokhande47100% (1)
- Plan for Inspection and Testing of LV Power CablesDokumen1 halamanPlan for Inspection and Testing of LV Power CablesRami KsidaBelum ada peringkat
- CV Template ReceptionistDokumen2 halamanCV Template ReceptionistMuhammad Waqas LatifBelum ada peringkat
- Bitsler DicebotDokumen4 halamanBitsler DicebotShinsBelum ada peringkat
- Elite FY'22 On Campus - SRM Institute of Science and Technology - Business Interview Schedule 29-Sep-21Dokumen40 halamanElite FY'22 On Campus - SRM Institute of Science and Technology - Business Interview Schedule 29-Sep-21aayush raghav (RA1811003020302)Belum ada peringkat
- MVC & Web Api - MCQ: Duration: 30mins Marks: 20Dokumen3 halamanMVC & Web Api - MCQ: Duration: 30mins Marks: 20ManuPcBelum ada peringkat
- 0751 VICTAULIC in Mechanical PipingDokumen17 halaman0751 VICTAULIC in Mechanical PipingsyafiqBelum ada peringkat
- Wind farm project NPV and LCOE analysisDokumen5 halamanWind farm project NPV and LCOE analysisPedro Galvani72% (32)
- Executive MBA Placement Brochure of IIM Bangalore PDFDokumen48 halamanExecutive MBA Placement Brochure of IIM Bangalore PDFnIKKOOBelum ada peringkat
- GLARE - History of The Development of A New Aircraft MaterialDokumen229 halamanGLARE - History of The Development of A New Aircraft MaterialklausoshoBelum ada peringkat
- System Software Module 3Dokumen109 halamanSystem Software Module 3arunlaldsBelum ada peringkat