Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Ultimate Stretching GuideDokumen18 halamanUltimate Stretching GuideJason Collingburn100% (10)
- Significant Difference of Mean Prevalence of Systolic Blood Pressure in Terms of Body Mass IndexDokumen5 halamanSignificant Difference of Mean Prevalence of Systolic Blood Pressure in Terms of Body Mass IndexJesse Israel TadenaBelum ada peringkat
- Items: 17 Table Ware and Galley Utensils 1 - 69Dokumen5 halamanItems: 17 Table Ware and Galley Utensils 1 - 69Jesse Israel TadenaBelum ada peringkat
- Ebn RMCDokumen5 halamanEbn RMCJesse Israel TadenaBelum ada peringkat
- Full QXNR - 405Dokumen7 halamanFull QXNR - 405Jesse Israel TadenaBelum ada peringkat
- Statistical TXDokumen3 halamanStatistical TXJesse Israel TadenaBelum ada peringkat
- A. Inspects Skull For: Head-to-Toe AssessmentDokumen14 halamanA. Inspects Skull For: Head-to-Toe AssessmentJesse Israel TadenaBelum ada peringkat
- Reflection - Bill of RightDokumen1 halamanReflection - Bill of RightJesse Israel TadenaBelum ada peringkat
- RRL - Weight, AgeDokumen2 halamanRRL - Weight, AgeJesse Israel Tadena0% (1)
- Far Eastern University Institute of Nursing SY: 2013-2014Dokumen3 halamanFar Eastern University Institute of Nursing SY: 2013-2014Jesse Israel TadenaBelum ada peringkat
- Education and CertificationsDokumen5 halamanEducation and CertificationsJesse Israel TadenaBelum ada peringkat
- Accomplishment Report FinalDokumen4 halamanAccomplishment Report FinalJesse Israel TadenaBelum ada peringkat
- Socio-Anthropology: Despues, Andrea Louis T. January 22, 2014 BSN 701 Dr. Wilson S. ChuaDokumen2 halamanSocio-Anthropology: Despues, Andrea Louis T. January 22, 2014 BSN 701 Dr. Wilson S. ChuaJesse Israel TadenaBelum ada peringkat
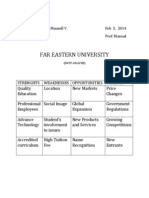
- Far Eastern University: W10 Mendoza, Nigel Lee Mansell V. Feb 5, 2014 IA12112 Prof. ManualDokumen1 halamanFar Eastern University: W10 Mendoza, Nigel Lee Mansell V. Feb 5, 2014 IA12112 Prof. ManualJesse Israel TadenaBelum ada peringkat
- Coppices Clonal Colonies Tree Height Measurement Tree Girth Measurement Tree Crown Measurement Tree Volume MeasurementDokumen1 halamanCoppices Clonal Colonies Tree Height Measurement Tree Girth Measurement Tree Crown Measurement Tree Volume MeasurementJesse Israel TadenaBelum ada peringkat
- Part of Body & Istilah Medis KeperawatanDokumen61 halamanPart of Body & Istilah Medis KeperawatanFholsen FrohansenBelum ada peringkat
- Orthopedic Nursing. Lecture Notes at Philipine Orthopedic CenterDokumen7 halamanOrthopedic Nursing. Lecture Notes at Philipine Orthopedic Centerhannjazz100% (5)
- Basic FESS - Step-By-Step Guide With Surgical Videos PDFDokumen20 halamanBasic FESS - Step-By-Step Guide With Surgical Videos PDFMujeeb MohammedBelum ada peringkat
- Anatomy Exam IIIDokumen8 halamanAnatomy Exam IIIJonathanBelum ada peringkat
- What Is The Epidermis PDFDokumen4 halamanWhat Is The Epidermis PDFlamarkaydotBelum ada peringkat
- Upon Inspecting, It Is: Inspect For The ColorDokumen5 halamanUpon Inspecting, It Is: Inspect For The ColorshakesBelum ada peringkat
- Urologic Surgery BOOK Sabiston Textbook of Surgery, Twentieth Edition Townsend, Courtney M., JR., Beauchamp, R. Daniel Evers, B. Mark, Mattox, Kenneth LDokumen39 halamanUrologic Surgery BOOK Sabiston Textbook of Surgery, Twentieth Edition Townsend, Courtney M., JR., Beauchamp, R. Daniel Evers, B. Mark, Mattox, Kenneth Loeij stevanus WijayaBelum ada peringkat
- Knowing Your Body: Conversation Cheat SheetDokumen2 halamanKnowing Your Body: Conversation Cheat SheetClarisse Joyce GenerBelum ada peringkat
- Chapter - 2 Nutrition in Animals Digestion in HumansDokumen6 halamanChapter - 2 Nutrition in Animals Digestion in HumansGeeta BhattBelum ada peringkat
- Physical Therapy Protocols - Knee ConditionsDokumen120 halamanPhysical Therapy Protocols - Knee Conditionssayles4174100% (1)
- Bio 201 - Bone Practical Part 1 (Axial Skeleton)Dokumen5 halamanBio 201 - Bone Practical Part 1 (Axial Skeleton)Gretchen100% (1)
- Science 10 Activity Sheet Male and Female Reproductive SystemDokumen2 halamanScience 10 Activity Sheet Male and Female Reproductive SystemKarl BadolesBelum ada peringkat
- Anatomy 2022Dokumen7 halamanAnatomy 2022Rayane NaegelsBelum ada peringkat
- 14 Sop Got Electric ShockDokumen3 halaman14 Sop Got Electric ShockRio SimatupangBelum ada peringkat
- Mcqs Nervuos SystemDokumen4 halamanMcqs Nervuos Systemaslam jan100% (2)
- Yoga Pose PacketDokumen10 halamanYoga Pose Packetapi-338710241Belum ada peringkat
- By Tracy KuhnDokumen33 halamanBy Tracy KuhnMae T OlivaBelum ada peringkat
- Controversies in Lower-Extremity AmputationDokumen12 halamanControversies in Lower-Extremity AmputationEGBelum ada peringkat
- ReflexesDokumen37 halamanReflexesmishky19Belum ada peringkat
- Saladin: Anatomy & Physiology: The Unity of Form and Function, Third Edition Front Matter Clinical EmphasisDokumen3 halamanSaladin: Anatomy & Physiology: The Unity of Form and Function, Third Edition Front Matter Clinical EmphasisJelena PopovićBelum ada peringkat
- 3 Bagua Internal Warm-Up MethodDokumen65 halaman3 Bagua Internal Warm-Up Methodvincraig100% (2)
- Spinal Cord InjuryDokumen44 halamanSpinal Cord InjuryMohd Farid Bin RosliBelum ada peringkat
- The Neutral Zone Concept in Complete DentureDokumen122 halamanThe Neutral Zone Concept in Complete Denturevahini niharikaBelum ada peringkat
- 神經學檢查Dokumen3 halaman神經學檢查api-19521590100% (1)
- Ultrasound-Guided Lumbar Selective Nerve Root BlockDokumen12 halamanUltrasound-Guided Lumbar Selective Nerve Root BlockmirnaBelum ada peringkat
- InfographicDokumen1 halamanInfographicmaricarBelum ada peringkat
- Bio E1 Chapter 2 PDFDokumen26 halamanBio E1 Chapter 2 PDFToto lstBelum ada peringkat
- Difference Between Primary and Permanent TeethDokumen15 halamanDifference Between Primary and Permanent TeetharthisaBelum ada peringkat
- Overview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionDokumen10 halamanOverview of Cardiovascular System: An Introduction To Chapters 9 - 24 and Chapter 36 Guyton and Hall, 12 EditionbahahahahBelum ada peringkat