Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- ADHD Parent Questionnaire PDFDokumen4 halamanADHD Parent Questionnaire PDFklichtBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Clemson University Power ProgramDokumen6 halamanClemson University Power ProgramcoachrocBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Rhinoplasty Dissection ManualDokumen185 halamanRhinoplasty Dissection ManualVikas Vats100% (3)
- Important Question For Dialysis TechnicianDokumen7 halamanImportant Question For Dialysis Technicianhunbaitmiki hinge100% (1)
- The Fitness Project 2018Dokumen34 halamanThe Fitness Project 2018San joe50% (2)
- Guidelines Emergency Medicine Pharmacist ServicesDokumen15 halamanGuidelines Emergency Medicine Pharmacist ServicesMárcio BatistaBelum ada peringkat
- Nursing Care Plan Mobility SampleDokumen6 halamanNursing Care Plan Mobility Samplen2biologyBelum ada peringkat
- Acute Effects of Radiation InjuryDokumen8 halamanAcute Effects of Radiation InjuryVikas VatsBelum ada peringkat
- Design Manual - Municipal Wastewater DisinfectionDokumen264 halamanDesign Manual - Municipal Wastewater DisinfectionPillaca Ugarte Ulises RansesBelum ada peringkat
- Practice HPIDokumen3 halamanPractice HPImedicalmatins100% (1)
- Reflexology and DementiaDokumen8 halamanReflexology and DementiaNatalie Stubbs100% (1)
- Sinew Channels by J Yuen002Dokumen81 halamanSinew Channels by J Yuen002Jonathan100% (1)
- Clinical Pharmacy PractiseDokumen28 halamanClinical Pharmacy Practise081546579656Belum ada peringkat
- TG-43 ArDokumen68 halamanTG-43 ArCecilia Querebalu Garcia0% (1)
- Standard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCDokumen4 halamanStandard Operating Procedure Handling, Storage and Disposal: Punyam Manufacturing INCJaijeev PaliBelum ada peringkat
- Facial AnatomyDokumen11 halamanFacial AnatomySneha SthaBelum ada peringkat
- Alternative Method For Fabrication of Power ArmDokumen2 halamanAlternative Method For Fabrication of Power ArmVikas VatsBelum ada peringkat
- Evoked PotentialDokumen6 halamanEvoked PotentialVikas VatsBelum ada peringkat
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDokumen17 halamanPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsBelum ada peringkat
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDokumen2 halamanBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDokumen6 halamanVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsBelum ada peringkat
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDokumen7 halamanHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsBelum ada peringkat
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Dokumen5 halaman1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsBelum ada peringkat
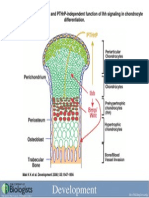
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Dokumen1 halamanDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsBelum ada peringkat
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDokumen9 halamanComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsBelum ada peringkat
- B PharmacyDokumen26 halamanB PharmacyAkankshaBelum ada peringkat
- Name of Drug SoludexideDokumen2 halamanName of Drug SoludexideSian AsadaBelum ada peringkat
- Glibenclamide MSDSDokumen3 halamanGlibenclamide MSDSOdunlamiBelum ada peringkat
- Chlinical Pharmacokinetics On Renal Failure PatientsDokumen29 halamanChlinical Pharmacokinetics On Renal Failure PatientsDenadaPutriBelum ada peringkat
- Dementia AssignmentDokumen19 halamanDementia AssignmentVandna Vikram Novlani50% (2)
- Dozois 5e Chapter05 TIFDokumen22 halamanDozois 5e Chapter05 TIFrebeccaBelum ada peringkat
- Oral Preparations: Erdosteine ZertinDokumen4 halamanOral Preparations: Erdosteine ZertinmagreaBelum ada peringkat
- Introduction To Environmental EngineeringDokumen41 halamanIntroduction To Environmental EngineeringPaul Santos NonatBelum ada peringkat
- FMRI Obs Icu & HduDokumen13 halamanFMRI Obs Icu & HduApoorv JainBelum ada peringkat
- ENLS V4.0 ME Manuscript FINALDokumen17 halamanENLS V4.0 ME Manuscript FINALkoko komarudinBelum ada peringkat
- Mental Health Act Ten LawDokumen8 halamanMental Health Act Ten LawAbigail BrillantesBelum ada peringkat
- 2023 Vein AnatomyDokumen6 halaman2023 Vein AnatomyKarenBelum ada peringkat
- Fgi Guidelines 2014 Hop TocDokumen10 halamanFgi Guidelines 2014 Hop TocZaw Moe KhineBelum ada peringkat
- The Effect of Pilates Based Exercise On Mobility, Postural Stability, and Balance in Order To Decrease Fall Risk in Older AdultsDokumen7 halamanThe Effect of Pilates Based Exercise On Mobility, Postural Stability, and Balance in Order To Decrease Fall Risk in Older AdultsMuhammad Cholid AlfahroziBelum ada peringkat
- HIV Policy MemoDokumen3 halamanHIV Policy MemoZhihong XuBelum ada peringkat
- Abnormal Psychology Notes: Anxiety DisordersDokumen4 halamanAbnormal Psychology Notes: Anxiety DisordersAshley ChenenBelum ada peringkat
- Post Op Management Following Surgery For Rectal ProlapseDokumen2 halamanPost Op Management Following Surgery For Rectal ProlapseChris NewallBelum ada peringkat