Anda mungkin juga menyukai
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamDari EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamPenilaian: 5 dari 5 bintang5/5 (1)
- ACLS Pocket GuideDokumen5 halamanACLS Pocket Guidedragnu100% (1)
- Emergency Parenteral Drugs ListDokumen4 halamanEmergency Parenteral Drugs ListRem Remoreras75% (4)
- List of Pharmaceutical Companies in PuneDokumen5 halamanList of Pharmaceutical Companies in PuneMohan Babu100% (1)
- Chronic Pain Management ChartsDokumen2 halamanChronic Pain Management Chartslrpokhrel100% (3)
- Pharmacy Business Requirements (Philippines) Pinoy PharmacistsDokumen4 halamanPharmacy Business Requirements (Philippines) Pinoy PharmacistsJohnny Manahan100% (1)
- Warning: Use at Your Own RiskDokumen4 halamanWarning: Use at Your Own RiskAhmed ZakariaBelum ada peringkat
- 5H 5TDokumen4 halaman5H 5TFelicia SutarliBelum ada peringkat
- Eclampsia-Icu Management ProtocolDokumen3 halamanEclampsia-Icu Management ProtocolmatentenBelum ada peringkat
- ACLS Drugs&Drips Final PDFDokumen6 halamanACLS Drugs&Drips Final PDFmesrianti_rubenBelum ada peringkat
- Updates American Heart Association Cardiopulmonary Resuscitation GuidelineDokumen32 halamanUpdates American Heart Association Cardiopulmonary Resuscitation GuidelineramzishindiBelum ada peringkat
- ICU DrugsDokumen1 halamanICU DrugsMimiBelum ada peringkat
- ECSI CAAlgorithm PDFDokumen2 halamanECSI CAAlgorithm PDFCarlos ChiBelum ada peringkat
- IVIG RateDokumen2 halamanIVIG RatelydiasusantiBelum ada peringkat
- DiltiazemDokumen2 halamanDiltiazemphat lippBelum ada peringkat
- Epinephrine Dosing, Indications, Interactions, Adverse Effects, and MoreDokumen4 halamanEpinephrine Dosing, Indications, Interactions, Adverse Effects, and MoreApuntesdemedicinaa blog100% (1)
- Adult Advanced Life Support2Dokumen34 halamanAdult Advanced Life Support2drDilanBelum ada peringkat
- Dosage Midazolam PDFDokumen7 halamanDosage Midazolam PDFIrsani FeniliaBelum ada peringkat
- KetamineDokumen5 halamanKetamineapi-142637023Belum ada peringkat
- 2005 ACLS Guidelines 5.15Dokumen11 halaman2005 ACLS Guidelines 5.15gr8_nurseBelum ada peringkat
- AntidotesDokumen36 halamanAntidotesMohamed Haggag100% (1)
- Lsuhsc Nursing Licensed Personnel Inpatient RN Pharmacology Exam InstructionsDokumen10 halamanLsuhsc Nursing Licensed Personnel Inpatient RN Pharmacology Exam Instructionskellly100% (1)
- Essenc I Al TherapyDokumen9 halamanEssenc I Al TherapyFabian Ramirez HincapiéBelum ada peringkat
- Anaesthetic Drugs Cheat SheetsDokumen2 halamanAnaesthetic Drugs Cheat SheetsPkern100% (3)
- Pneumonics For AclsDokumen2 halamanPneumonics For Aclskrishnaprasadm7100% (2)
- EpinephrineDokumen4 halamanEpinephrineHarthwell CapistranoBelum ada peringkat
- Adrenaline 1 MG Intravenously Should Be Given Every: Hints and Tips For The ExamDokumen1 halamanAdrenaline 1 MG Intravenously Should Be Given Every: Hints and Tips For The ExamJennyBelum ada peringkat
- ACLS Simplify AlgorithmDokumen6 halamanACLS Simplify AlgorithmKristine Monforte Coma UritaBelum ada peringkat
- DripsDokumen52 halamanDripsjanoloBelum ada peringkat
- CVS Dental ConsiderationsDokumen20 halamanCVS Dental ConsiderationsSamii ShkBelum ada peringkat
- Medication Administration PolicyDokumen188 halamanMedication Administration Policyليراث ليBelum ada peringkat
- Drug Calculations SolutionsDokumen4 halamanDrug Calculations SolutionsBigTam1981100% (2)
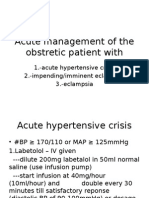
- Acute Management of The Obstretic Patient WithDokumen7 halamanAcute Management of The Obstretic Patient WithMahes WarBelum ada peringkat
- Math For Meds FinalDokumen7 halamanMath For Meds FinalA BravoBelum ada peringkat
- Advanced IV-Metrology F090Dokumen17 halamanAdvanced IV-Metrology F090grayburn_1Belum ada peringkat
- Idiot NotesDokumen53 halamanIdiot NotesRay PerezBelum ada peringkat
- Elsharnoby Pediatric Made EasyDokumen160 halamanElsharnoby Pediatric Made Easyelmaadawy20020% (1)
- Advanced Cardiac Life Support PDFDokumen9 halamanAdvanced Cardiac Life Support PDFYulias YoweiBelum ada peringkat
- Quiz-OB Surgical-FinalsDokumen3 halamanQuiz-OB Surgical-FinalsMadel CagandeBelum ada peringkat
- CRASH CART Presentation PPTX 1 MELODokumen33 halamanCRASH CART Presentation PPTX 1 MELOCamille GalasBelum ada peringkat
- Thrombolytic TherapyDokumen16 halamanThrombolytic TherapyAnonymous nrZXFwBelum ada peringkat
- Pharma Act 6Dokumen7 halamanPharma Act 6Shade ElugbajuBelum ada peringkat
- Treatment MGRDokumen12 halamanTreatment MGRMod AntbugBelum ada peringkat
- Frank Shann - 040315153700Dokumen63 halamanFrank Shann - 040315153700juwitapratiwiBelum ada peringkat
- Algoritm Trat Algoritm Tratament Astm Bronsic - Pdfament Astm BronsicDokumen1 halamanAlgoritm Trat Algoritm Tratament Astm Bronsic - Pdfament Astm BronsicSbarcea AurelBelum ada peringkat
- Perkembangan Baru Resusitasi Jantung ParuDokumen27 halamanPerkembangan Baru Resusitasi Jantung ParuMarcelina Aprisia PrimadiBelum ada peringkat
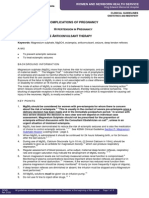
- Complications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapyDokumen8 halamanComplications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapysucyasyifaBelum ada peringkat
- DrugDokumen3 halamanDrugkhangsiean89100% (1)
- Infusions in CCU 2Dokumen1 halamanInfusions in CCU 2MimiBelum ada peringkat
- The Drug Doses in The Following Pages Are ReproducDokumen168 halamanThe Drug Doses in The Following Pages Are ReproducAsghar ShahBelum ada peringkat
- Drug Fluids CalculationDokumen23 halamanDrug Fluids CalculationRuby Jane Mansueto - Pague100% (1)
- Drugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaDokumen20 halamanDrugs and Defibrillation: Department of Anesthesiology & Reanimation General Hospital TasikmalayaAfrida Sahestina100% (1)
- Management of Anesthesia: Diabetes MellitusDokumen29 halamanManagement of Anesthesia: Diabetes MellitusHari PrasadBelum ada peringkat
- The Crash CartDokumen39 halamanThe Crash Cartpramod kumawat100% (1)
- Dimensional Analysis For Nursing StudentsDari EverandDimensional Analysis For Nursing StudentsBelum ada peringkat
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesDari EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesPenilaian: 4 dari 5 bintang4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesDari EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesPenilaian: 5 dari 5 bintang5/5 (2)
- Heart of the Field "Refresher & Nha Certification Quick Notes"Dari EverandHeart of the Field "Refresher & Nha Certification Quick Notes"Belum ada peringkat
- Confessio Fraternitatis - AnonymousDokumen9 halamanConfessio Fraternitatis - AnonymousАлександар ПејчићBelum ada peringkat
- TamaraKosticNRT6708 BiggerDokumen24 halamanTamaraKosticNRT6708 BiggerАлександар ПејчићBelum ada peringkat
- Atrijalna Fibrilacija I FlaterDokumen3 halamanAtrijalna Fibrilacija I FlaterАлександар ПејчићBelum ada peringkat
- Torsade de Pointes (Polymorphic Ventricular Tachycardia)Dokumen1 halamanTorsade de Pointes (Polymorphic Ventricular Tachycardia)Александар ПејчићBelum ada peringkat
- Pharma 7Dokumen5 halamanPharma 7Uday kumarBelum ada peringkat
- Formulation and Process Optimization of Glimepiride Tablets: Original ArticlesDokumen9 halamanFormulation and Process Optimization of Glimepiride Tablets: Original ArticlesMuhammad ZubairBelum ada peringkat
- EtoposideDokumen3 halamanEtoposideNoamiBelum ada peringkat
- Rko 2019Dokumen218 halamanRko 2019SahrilBelum ada peringkat
- Dapoxetine Hydrochloride Prescribing InformationDokumen17 halamanDapoxetine Hydrochloride Prescribing InformationAdnan TowfiqueBelum ada peringkat
- Lecture # 8 Dr. Laiq (6.10.19) PDFDokumen50 halamanLecture # 8 Dr. Laiq (6.10.19) PDFAbbas HassanBelum ada peringkat
- Master Obat FarmasiDokumen75 halamanMaster Obat FarmasiSiska PrasenjaBelum ada peringkat
- UNIT 1 Computer 23 PDFDokumen7 halamanUNIT 1 Computer 23 PDFHayna RoseBelum ada peringkat
- Admin,+journal+manager,+70 AJPCR 21211 RA QueryDokumen4 halamanAdmin,+journal+manager,+70 AJPCR 21211 RA QueryTareq Al MahmudBelum ada peringkat
- Mesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidDokumen4 halamanMesalazine: Mesalazine (INN, BAN), Also Known As Mesalamine (USAN) or 5-Aminosalicylic AcidAnkan PalBelum ada peringkat
- How To Calculate Standard Patent Expiry Dates and Data ExclusivityDokumen9 halamanHow To Calculate Standard Patent Expiry Dates and Data ExclusivityAnuj MairhBelum ada peringkat
- DILADokumen1.369 halamanDILALilly Hoo LeeBelum ada peringkat
- Egypt Biosimilar Guidline Biologicals RegistrationDokumen54 halamanEgypt Biosimilar Guidline Biologicals Registrationshivani hiremathBelum ada peringkat
- Drug Infusion Guide For SORT PDFDokumen5 halamanDrug Infusion Guide For SORT PDFAli HasanBelum ada peringkat
- For Original and Supplemental New Animal Drug Applications PDFDokumen20 halamanFor Original and Supplemental New Animal Drug Applications PDFMichael wangBelum ada peringkat
- NotaDokumen17 halamanNotaimas apriyantiBelum ada peringkat
- Pha619 Lec Chap 2Dokumen9 halamanPha619 Lec Chap 2Grace HernandezBelum ada peringkat
- Clinical Veterinary PharmacologyDokumen4 halamanClinical Veterinary PharmacologyLaureece Salm ApduhanBelum ada peringkat
- LIST of E-Books On Perpetual Access On IP/MHRD WIFIDokumen2 halamanLIST of E-Books On Perpetual Access On IP/MHRD WIFIRaj Kumar SoniBelum ada peringkat
- Student Engagement 222Dokumen5 halamanStudent Engagement 222Danial IqhwanBelum ada peringkat
- Domperidone Vs MetoclopramideDokumen5 halamanDomperidone Vs MetoclopramideJuly BerybeBelum ada peringkat
- D Pharmacy SyllabusDokumen2 halamanD Pharmacy SyllabusRitesh PandeyBelum ada peringkat
- MedicationsDokumen2 halamanMedicationsHanna SeBelum ada peringkat
- Rifampicin-An Overview: Available Online atDokumen5 halamanRifampicin-An Overview: Available Online atyeseniasaviraBelum ada peringkat
- Ho6a Assist V 3.1 For Health ProfessionalsDokumen5 halamanHo6a Assist V 3.1 For Health ProfessionalsDetti FahmiasyariBelum ada peringkat
- Dafus PenilitianDokumen5 halamanDafus PenilitianDim YotaBelum ada peringkat
- Lab 1 (Lمحاضرات العملي)Dokumen20 halamanLab 1 (Lمحاضرات العملي)RaghdaBelum ada peringkat