Anda mungkin juga menyukai
- (Oaci / Rtari) : Manual de Estudio para La Preparacion Del Examen de Competencia Lingüística OaciDokumen29 halaman(Oaci / Rtari) : Manual de Estudio para La Preparacion Del Examen de Competencia Lingüística OaciAziel Ontiveros Mtz.Belum ada peringkat
- Case Study DecompressionDokumen18 halamanCase Study Decompressiona320Belum ada peringkat
- Normal Checklist: AirbusDokumen2 halamanNormal Checklist: AirbusAwiatorzy WielcyBelum ada peringkat
- Tenerife Airport DisasterDokumen14 halamanTenerife Airport DisasterEzaniKhaezuranBelum ada peringkat
- Aviation Human Factors Industry News 05Dokumen22 halamanAviation Human Factors Industry News 05Adriano MoralesBelum ada peringkat
- Flight Safety Article FLT LT SoumitraDokumen4 halamanFlight Safety Article FLT LT SoumitraSälmän Md ÄhsänBelum ada peringkat
- Why Did You Choose To Become A Pilot?: Thrust LeversDokumen8 halamanWhy Did You Choose To Become A Pilot?: Thrust LeversJonasBelum ada peringkat
- Effective Communication in The Aviation Environment: Work in ProgressDokumen4 halamanEffective Communication in The Aviation Environment: Work in ProgressIuliia FilipBelum ada peringkat
- Aviation EnglishDokumen86 halamanAviation Englishtmhoangvna100% (1)
- Business Start-Up 2-Student 39 S Book-18Dokumen4 halamanBusiness Start-Up 2-Student 39 S Book-18Bayu beningBelum ada peringkat
- Probable Hazard in AviationDokumen6 halamanProbable Hazard in AviationPrinnia Zulfiqur BorshaBelum ada peringkat
- 1.) Always Make Yourself Clearly Understood. 2.) Always Comply Promptly and Correctly With ATCDokumen31 halaman1.) Always Make Yourself Clearly Understood. 2.) Always Comply Promptly and Correctly With ATCRoger SacchelliBelum ada peringkat
- Air France 447Dokumen11 halamanAir France 447sekarjoshuaBelum ada peringkat
- Bird Strike ThesisDokumen7 halamanBird Strike Thesisarianadavishighpoint100% (2)
- Safety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 6 Situational AwarenessDokumen20 halamanSafety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 6 Situational AwarenessSonya McSharkBelum ada peringkat
- Sentinel Name Change: Safety@capnhq - GovDokumen8 halamanSentinel Name Change: Safety@capnhq - Govcapok113Belum ada peringkat
- Safety Awareness: Celebrating Operational ExcellenceDokumen8 halamanSafety Awareness: Celebrating Operational ExcellenceMario AndrewBelum ada peringkat
- Airplane Accident Research PaperDokumen5 halamanAirplane Accident Research Paperyelbsyvkg100% (1)
- Picture 4 - Mean Landing Gear RetractedDokumen3 halamanPicture 4 - Mean Landing Gear RetractedDaniel RodriguesBelum ada peringkat
- 3a The Truth About Air TravelDokumen40 halaman3a The Truth About Air TravelRamiro BritoBelum ada peringkat
- Jeffco Squadron - Dec 2008Dokumen14 halamanJeffco Squadron - Dec 2008CAP Unit NewslettersBelum ada peringkat
- Research Paper Topics On Airplane AccidentsDokumen7 halamanResearch Paper Topics On Airplane Accidentsjssoulznd100% (1)
- Trabalho Inglês Aplicado À Aviação IVDokumen3 halamanTrabalho Inglês Aplicado À Aviação IVCadu ViveirosBelum ada peringkat
- Fear of FlyingDokumen12 halamanFear of FlyingTommaso RusmiBelum ada peringkat
- Cabin Crew Interview Question & Answers: 1) Explain What Is Air Turbulence?Dokumen19 halamanCabin Crew Interview Question & Answers: 1) Explain What Is Air Turbulence?Pargat Singh100% (2)
- Callback - NASA - 492Dokumen2 halamanCallback - NASA - 492Αλέξανδρος ΒασιλειάδηςBelum ada peringkat
- Fat Bird Hath A Fall Part 1 V-IfDokumen12 halamanFat Bird Hath A Fall Part 1 V-IfShantanu SoodBelum ada peringkat
- Safety Compass March 2014Dokumen5 halamanSafety Compass March 2014rotorbrentBelum ada peringkat
- Operations Attachment 22 - Atlas CRM Training PresentationDokumen56 halamanOperations Attachment 22 - Atlas CRM Training PresentationGFBelum ada peringkat
- Success of CRMDokumen7 halamanSuccess of CRMSayandeep karBelum ada peringkat
- Eol 3Dokumen3 halamanEol 3api-632633923Belum ada peringkat
- Thesis About Plane CrashDokumen7 halamanThesis About Plane Crashlniaxfikd100% (2)
- WB Unit 5 Comy Fly With UsDokumen4 halamanWB Unit 5 Comy Fly With UsNastya Volod'koBelum ada peringkat
- Air France 447 PDFDokumen11 halamanAir France 447 PDFafonsogonBelum ada peringkat
- Army Aviation Digest - Jun 1960Dokumen40 halamanArmy Aviation Digest - Jun 1960Aviation/Space History Library100% (1)
- What Air Crash Investigations Didn't Tell You About QF32 (Airbus A380)Dokumen8 halamanWhat Air Crash Investigations Didn't Tell You About QF32 (Airbus A380)Thavam RatnaBelum ada peringkat
- Pell City Squadron - Oct 2009Dokumen5 halamanPell City Squadron - Oct 2009CAP Unit NewslettersBelum ada peringkat
- Aef 3aDokumen7 halamanAef 3aarezouBelum ada peringkat
- Airplane Accidents Research PaperDokumen7 halamanAirplane Accidents Research Paperc9spy2qz100% (1)
- Assuring Safer Skies? - A Survey of Aeromedical Issues Post-GermanDokumen27 halamanAssuring Safer Skies? - A Survey of Aeromedical Issues Post-GermanWiraBelum ada peringkat
- Midterm Seatwork #1Dokumen2 halamanMidterm Seatwork #1Charlene SibayanBelum ada peringkat
- Asl 2019 02Dokumen26 halamanAsl 2019 02John DalleyBelum ada peringkat
- Tours and TravelDokumen4 halamanTours and TravelMichael S. Muli Jr.Belum ada peringkat
- 213 - en VIsual Collision AvoidanceDokumen16 halaman213 - en VIsual Collision AvoidancepksdfBelum ada peringkat
- Eplis RCC AzDokumen18 halamanEplis RCC AzDenis SantosBelum ada peringkat
- Wa0033.Dokumen26 halamanWa0033.Akash MadniBelum ada peringkat
- Sorular LEVEL4Dokumen12 halamanSorular LEVEL4Tayfun TUNAERBelum ada peringkat
- Fluency and Interaction Booklet - Useful SentencesDokumen12 halamanFluency and Interaction Booklet - Useful Sentencestfz8x7hw2tBelum ada peringkat
- Human Factors For Aircraft MaintenanceDokumen97 halamanHuman Factors For Aircraft Maintenancemakree100% (1)
- The Bedrock Principles: DisciplineDokumen9 halamanThe Bedrock Principles: Disciplinekriki_mBelum ada peringkat
- Confessions of an Air Craft Pilot: Including Tales from the Pilot’s SeatDari EverandConfessions of an Air Craft Pilot: Including Tales from the Pilot’s SeatPenilaian: 1 dari 5 bintang1/5 (1)
- Professional Air Man ShipDokumen49 halamanProfessional Air Man Shipstanchell100% (2)
- Group 10 - TPDokumen5 halamanGroup 10 - TPJayce SiosonBelum ada peringkat
- Pell City Squadron - Apr 2012Dokumen18 halamanPell City Squadron - Apr 2012CAP Unit Newsletters100% (1)
- Pell City Squadron - Sep 2011Dokumen14 halamanPell City Squadron - Sep 2011CAP Unit NewslettersBelum ada peringkat
- How To Be A Better Pilot PDFDokumen48 halamanHow To Be A Better Pilot PDFTayfun TUNAER100% (1)
- IChemE - TCE - Top Five Facts Everyone Should Know About Oil ExplorationDokumen4 halamanIChemE - TCE - Top Five Facts Everyone Should Know About Oil Explorationsl1828Belum ada peringkat
- IChemE - TCE - To Err Is HumanDokumen2 halamanIChemE - TCE - To Err Is Humansl1828Belum ada peringkat
- Toolbox Talk - Lightning StrikesDokumen1 halamanToolbox Talk - Lightning Strikessl1828Belum ada peringkat
- Confirmation Bias - What You Can DoDokumen9 halamanConfirmation Bias - What You Can Dosl1828Belum ada peringkat
- Toolbox Talk - Safety Around High VoltageDokumen1 halamanToolbox Talk - Safety Around High Voltagesl1828Belum ada peringkat
- Toolbox Talk - Mounting and Dismounting EquipmentDokumen1 halamanToolbox Talk - Mounting and Dismounting Equipmentsl1828Belum ada peringkat
- Toolbox Talk - Means of EgressDokumen1 halamanToolbox Talk - Means of Egresssl1828Belum ada peringkat
- Food & Drink: Case Study: UnileverDokumen3 halamanFood & Drink: Case Study: Unileversl1828Belum ada peringkat
- CSB - Summary of Explosive & Toxic Incident Recommendations (1998-2013)Dokumen32 halamanCSB - Summary of Explosive & Toxic Incident Recommendations (1998-2013)sl1828Belum ada peringkat
- IChemE - XX-2008-Paper-11 - Bunding at Buncefield - Successes, Failures & Lessons LearnedDokumen13 halamanIChemE - XX-2008-Paper-11 - Bunding at Buncefield - Successes, Failures & Lessons Learnedsl1828Belum ada peringkat
- CEFIC - Measuring & Managing Co2 Emissions of European Chemical TransportDokumen40 halamanCEFIC - Measuring & Managing Co2 Emissions of European Chemical Transportsl1828Belum ada peringkat
- Battery Care and Tips2Dokumen1 halamanBattery Care and Tips2SCCstudent99Belum ada peringkat
- Toolbox Talk - Fume Hood DecommissionDokumen3 halamanToolbox Talk - Fume Hood Decommissionsl1828Belum ada peringkat
- Report of Inspection, Testing & Maintenance of Fire Pump AssembliesDokumen6 halamanReport of Inspection, Testing & Maintenance of Fire Pump Assembliessl1828100% (1)
- Toolbox Talk - Fume Hood RepairDokumen3 halamanToolbox Talk - Fume Hood Repairsl1828Belum ada peringkat
- CSB - Digest - Herrig Brothers - Propane Tank Explosion (1998)Dokumen2 halamanCSB - Digest - Herrig Brothers - Propane Tank Explosion (1998)sl1828Belum ada peringkat
- CSB Digest Union Carbide Nitrogen Asphyxiation (1998)Dokumen2 halamanCSB Digest Union Carbide Nitrogen Asphyxiation (1998)sl1828Belum ada peringkat
- Chemical Engineering - Hazardous Area ClassificationDokumen1 halamanChemical Engineering - Hazardous Area Classificationsl1828Belum ada peringkat
- CSB Digest West Pharmaceutical Dust Explosion (2003)Dokumen2 halamanCSB Digest West Pharmaceutical Dust Explosion (2003)sl1828Belum ada peringkat
- CEFIC Guidelines Transport Equipment Packed Cargo (2010)Dokumen7 halamanCEFIC Guidelines Transport Equipment Packed Cargo (2010)sl1828Belum ada peringkat
- CEFIC - ICE-Distribution Emergency Response Guidelines For Use by The Chemical Industry (2011)Dokumen15 halamanCEFIC - ICE-Distribution Emergency Response Guidelines For Use by The Chemical Industry (2011)sl1828Belum ada peringkat
- Safety Performance Based On Iogp PDFDokumen152 halamanSafety Performance Based On Iogp PDFAJMBelum ada peringkat
- Death in Dark CollectionDokumen45 halamanDeath in Dark CollectionEdward HumesBelum ada peringkat
- NTSB Plane Crash ReportDokumen4 halamanNTSB Plane Crash ReportPat ThomasBelum ada peringkat
- Safety ReportDokumen54 halamanSafety ReportDinesh PoudelBelum ada peringkat
- SimuladorDokumen4 halamanSimuladorPaco Iglesias CubilesBelum ada peringkat
- The MH370 TragedyDokumen21 halamanThe MH370 TragedyHuong Tra LeBelum ada peringkat
- Emirates Boeing 777 CrashDokumen4 halamanEmirates Boeing 777 CrashRahul RajanBelum ada peringkat
- NTSB Report On Crash Near ScioDokumen3 halamanNTSB Report On Crash Near ScioSinclair Broadcast Group - EugeneBelum ada peringkat
- Aviation English History and PedagogyDokumen9 halamanAviation English History and Pedagogydionicio perezBelum ada peringkat
- Aircraft Accident Report and Executive SummaryDokumen10 halamanAircraft Accident Report and Executive SummaryakeelBelum ada peringkat
- Auburndale Plane Crash NTSB Preliminary ReportDokumen2 halamanAuburndale Plane Crash NTSB Preliminary ReportCharles FrazierBelum ada peringkat
- AicDokumen1 halamanAicRajesh SahaniBelum ada peringkat
- OccurenceReport UPI6208Dokumen47 halamanOccurenceReport UPI6208danialomidvar100% (1)
- English Proficiency Test For Aviation Set 4Dokumen13 halamanEnglish Proficiency Test For Aviation Set 4Jivko Kostadinov67% (3)
- AviationDokumen27 halamanAviationAmar NathBelum ada peringkat
- BallisticDokumen7 halamanBallisticShaimah Rinda SariBelum ada peringkat
- "9 Keys To 9-11" by Nick Kollerstrom, PHDDokumen11 halaman"9 Keys To 9-11" by Nick Kollerstrom, PHDcentennia38Belum ada peringkat
- ComAir Flight 5191Dokumen3 halamanComAir Flight 5191Rajat JainBelum ada peringkat
- Contribution of Human Factors in Fatal Aircraft AccidentsDokumen3 halamanContribution of Human Factors in Fatal Aircraft AccidentsMaaz MoidBelum ada peringkat
- The Plane Paradox - More Automation Means More TrainingDokumen4 halamanThe Plane Paradox - More Automation Means More Trainingamit2810Belum ada peringkat
- Fly The Dog: Pilot Errors From A Pilot PerspectiveDokumen13 halamanFly The Dog: Pilot Errors From A Pilot PerspectiveIBooeingNG100% (1)
- Aviation Investigation ReportDokumen210 halamanAviation Investigation ReportepraetorianBelum ada peringkat
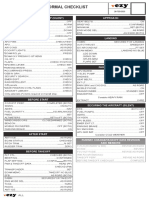
- Airbus A319 20 VEZY ChecklistDokumen2 halamanAirbus A319 20 VEZY ChecklistRobertBelum ada peringkat
- NASA: 71255main 03-021Dokumen2 halamanNASA: 71255main 03-021NASAdocumentsBelum ada peringkat
- Akasg 1Dokumen6 halamanAkasg 1Muhammad Arslan ShahBelum ada peringkat
- G-F-019 LIR LS Form Boeing 737-8-800Dokumen1 halamanG-F-019 LIR LS Form Boeing 737-8-800Georgios KumarcisBelum ada peringkat
- Airport Signs & MarkingsDokumen2 halamanAirport Signs & MarkingsAviation/Space History Library100% (5)
- Aviation Study Material - Sample Questions For RTR (A) Part 1 ExamDokumen6 halamanAviation Study Material - Sample Questions For RTR (A) Part 1 ExamRajesh67% (3)