Anda mungkin juga menyukai
- Jama Andersen 2017 Oi 160154Dokumen13 halamanJama Andersen 2017 Oi 160154HanyAbdallahBelum ada peringkat
- Balanced Crystalloids Versus Saline in Critically Ill AdultsDokumen11 halamanBalanced Crystalloids Versus Saline in Critically Ill AdultsbrquBelum ada peringkat
- Adjunctive Glucocorticoid Therapy in Patients With Septic ShockDokumen12 halamanAdjunctive Glucocorticoid Therapy in Patients With Septic Shockanggun pratissa100% (1)
- Quinn Incidence of HAP 2018Dokumen6 halamanQuinn Incidence of HAP 2018Sarah BeldinBelum ada peringkat
- Angiotensin II For The Treatment of Vasodilatory ShockDokumen12 halamanAngiotensin II For The Treatment of Vasodilatory ShockRoberto López MataBelum ada peringkat
- 10.1007/s00134 018 5085 0 PDFDokumen4 halaman10.1007/s00134 018 5085 0 PDFTiago SuaresBelum ada peringkat
- The Tiny Seed ResponseDokumen3 halamanThe Tiny Seed ResponseSarah BeldinBelum ada peringkat
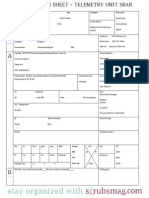
- Nurse Brain Sheet Telemetry Unit SBARDokumen1 halamanNurse Brain Sheet Telemetry Unit SBARvsosa624Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hip Interventions Project - Harris SvorinicDokumen3 halamanHip Interventions Project - Harris Svorinicapi-620069244Belum ada peringkat
- Pediatric Asthma Situation in Chengdu, China, During The COVID-19 Pandemic: An Observational StudyDokumen10 halamanPediatric Asthma Situation in Chengdu, China, During The COVID-19 Pandemic: An Observational StudyzainabBelum ada peringkat
- Managing Anaphylactic Shock Journal of Modern Pharmacy 2006Dokumen3 halamanManaging Anaphylactic Shock Journal of Modern Pharmacy 2006Saputro AbdiBelum ada peringkat
- Risk For Infection NCPDokumen2 halamanRisk For Infection NCPCharme Jean RaygonBelum ada peringkat
- Pentacam GuidelineDokumen43 halamanPentacam GuidelineEvelyn SepulvedaBelum ada peringkat
- Babylog® 8000 Plus Neonatal Intensive Care VentilationDokumen6 halamanBabylog® 8000 Plus Neonatal Intensive Care VentilationAGNIBelum ada peringkat
- Mini VET GuideDokumen186 halamanMini VET GuideemitibiBelum ada peringkat
- Drotaverine: Solution For Injection - 40 MG / 2 MLDokumen1 halamanDrotaverine: Solution For Injection - 40 MG / 2 MLZarbakht AliBelum ada peringkat
- Upper Respiratory Tract Infection (Farter Bu'RaraDokumen58 halamanUpper Respiratory Tract Infection (Farter Bu'RaraFajrul Fhalaq BasoBelum ada peringkat
- Malaria: Health Education HFT 201 By: Sophia Kol, MDDokumen10 halamanMalaria: Health Education HFT 201 By: Sophia Kol, MDTith SeavmeyBelum ada peringkat
- Cardiac Catheterization and Coronary Intervention (2nd Edition, 2020)Dokumen353 halamanCardiac Catheterization and Coronary Intervention (2nd Edition, 2020)John Cancel50% (2)
- Stok Opname Nopember 2015-RevisiDokumen146 halamanStok Opname Nopember 2015-RevisinooBelum ada peringkat
- Sports Injuries and AcupunctureDokumen19 halamanSports Injuries and AcupunctureLiliana Ponte100% (1)
- Invos System Improving Patient Outcomes Cerebral Somatic Oximetry BrochureDokumen6 halamanInvos System Improving Patient Outcomes Cerebral Somatic Oximetry Brochuremihalcea alinBelum ada peringkat
- Characterization of Successful Root Canal TreatmenDokumen10 halamanCharacterization of Successful Root Canal TreatmenSitiRahmahAzharBelum ada peringkat
- Cirrhosis & Vit KDokumen8 halamanCirrhosis & Vit KBagii GonchigBelum ada peringkat
- Axali, Damatebiti Tipobrivi Sagamocdo Testuri Sekitxvebi Medicinis Fakultetis Iii Kursis Studentebisatvis Mikrobiologia 2-SiDokumen15 halamanAxali, Damatebiti Tipobrivi Sagamocdo Testuri Sekitxvebi Medicinis Fakultetis Iii Kursis Studentebisatvis Mikrobiologia 2-SiMKGUBelum ada peringkat
- CV DR Ari Sami Hussain NadhimDokumen5 halamanCV DR Ari Sami Hussain NadhimAri SamiBelum ada peringkat
- NGT LavageDokumen16 halamanNGT LavageTina Alteran100% (1)
- History Taking Form in Gynecology Obstetrics - CompressDokumen8 halamanHistory Taking Form in Gynecology Obstetrics - CompresskeightBelum ada peringkat
- Access Corporate Fact SheetDokumen2 halamanAccess Corporate Fact SheetMattBelum ada peringkat
- Drug Study - LevetiracetamDokumen3 halamanDrug Study - LevetiracetamCath Bril100% (4)
- Pathophysiology ExaminationDokumen6 halamanPathophysiology ExaminationPractice Medi-nursingBelum ada peringkat
- DiabetesDokumen12 halamanDiabetessshiffanaBelum ada peringkat
- Antiviral Drugs PDFDokumen3 halamanAntiviral Drugs PDFKabisa MbetiBelum ada peringkat
- Hypokalemia - A Clinical UpdateDokumen12 halamanHypokalemia - A Clinical UpdateRushi PatelBelum ada peringkat
- ICF SwallowingDokumen2 halamanICF SwallowingMarcela Sanhueza GarridoBelum ada peringkat
- Bad Pharma - A Fraud in Clinical Trail DataDokumen27 halamanBad Pharma - A Fraud in Clinical Trail DataSimran WaghelaBelum ada peringkat
- Stroke Hemoragic: Sebagai Salah Satu Tugas Mata Kuliah TIK Akademi Keperawatan (Akper) SawerigadingDokumen10 halamanStroke Hemoragic: Sebagai Salah Satu Tugas Mata Kuliah TIK Akademi Keperawatan (Akper) SawerigadingMade Serly KrisdayantiBelum ada peringkat
- Medgears: We Have Been Pioneers at Manufacturing, Exporting and Wholesaling A Wide Assortment of High-QualityDokumen24 halamanMedgears: We Have Been Pioneers at Manufacturing, Exporting and Wholesaling A Wide Assortment of High-QualitySubhasis MallikBelum ada peringkat