Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- King Rush MoreDokumen1 halamanKing Rush MoreawuahbohBelum ada peringkat
- Oop Say You Know MeDokumen1 halamanOop Say You Know MeawuahbohBelum ada peringkat
- Pharm NclexDokumen9 halamanPharm NclexawuahbohBelum ada peringkat
- Article For CET CHFDokumen5 halamanArticle For CET CHFawuahbohBelum ada peringkat
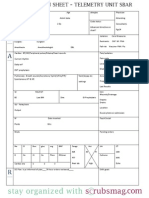
- Nurse Brain Sheet Telemetry Unit SBARDokumen1 halamanNurse Brain Sheet Telemetry Unit SBARvsosa624Belum ada peringkat
- Massachusetts Department of Public HealthDokumen24 halamanMassachusetts Department of Public HealthawuahbohBelum ada peringkat
- HandOff SampleToolsDokumen9 halamanHandOff SampleToolsOllie EvansBelum ada peringkat
- The BSN Job Search: Interview Preparation: Telling Your StoryDokumen25 halamanThe BSN Job Search: Interview Preparation: Telling Your StoryawuahbohBelum ada peringkat
- Article For JournalDokumen6 halamanArticle For JournalawuahbohBelum ada peringkat
- NCLEX Random FactsDokumen34 halamanNCLEX Random FactsLegnaMary100% (8)
- Probability of A or B and A and B-1Dokumen2 halamanProbability of A or B and A and B-1awuahbohBelum ada peringkat
- Middle Age Adult Health History Assignment Guidelines N315 Fall 2013Dokumen23 halamanMiddle Age Adult Health History Assignment Guidelines N315 Fall 2013awuahbohBelum ada peringkat
- EBP Article 1Dokumen11 halamanEBP Article 1awuahbohBelum ada peringkat
- PolypharmacyDokumen24 halamanPolypharmacySurina Zaman HuriBelum ada peringkat
- Drugs NclexDokumen30 halamanDrugs Nclexawuahboh100% (1)
- EBP Article 3Dokumen6 halamanEBP Article 3awuahbohBelum ada peringkat
- Tips On Answering NclexDokumen4 halamanTips On Answering NclexawuahbohBelum ada peringkat
- Random FactsDokumen338 halamanRandom Factscyram81100% (1)
- Critical Thinking StrategiesDokumen3 halamanCritical Thinking StrategiesawuahbohBelum ada peringkat
- Therapeutic CommunicationDokumen1 halamanTherapeutic CommunicationawuahbohBelum ada peringkat
- Does Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorDokumen24 halamanDoes Prospective Payment Increase Hospital (In) Efficiency? Evidence From The Swiss Hospital SectorawuahbohBelum ada peringkat
- ENT Throat and EsophagusDokumen41 halamanENT Throat and EsophagusMUHAMMAD HASAN NAGRABelum ada peringkat
- Parkland formula and rule of 9Dokumen8 halamanParkland formula and rule of 9awuahbohBelum ada peringkat
- STDA VaricealDokumen8 halamanSTDA VaricealDeisy de JesusBelum ada peringkat
- Article For CET CHFDokumen5 halamanArticle For CET CHFawuahbohBelum ada peringkat
- Article For Jouranal 2 (498P)Dokumen5 halamanArticle For Jouranal 2 (498P)awuahbohBelum ada peringkat
- Patient Report FormDokumen1 halamanPatient Report FormawuahbohBelum ada peringkat
- Debate 3 Youth Incarceration in Adult PrisonsDokumen6 halamanDebate 3 Youth Incarceration in Adult PrisonsawuahbohBelum ada peringkat
- Article For Journal 4-18-14Dokumen8 halamanArticle For Journal 4-18-14awuahbohBelum ada peringkat
- Article For JournalDokumen6 halamanArticle For JournalawuahbohBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Concept Map Draft ExampleDokumen2 halamanConcept Map Draft ExamplemeliBelum ada peringkat
- Exercise and Physical Activity For Older - VanBeveren 2012 PDFDokumen22 halamanExercise and Physical Activity For Older - VanBeveren 2012 PDFJuani CantellanosBelum ada peringkat
- BLS Adult Skills Checklist 2016Dokumen2 halamanBLS Adult Skills Checklist 2016Wahyudi QorahmanBelum ada peringkat
- PleuritisDokumen48 halamanPleuritisMuhammad FhaliqBelum ada peringkat
- EMS Drug DilutionDokumen21 halamanEMS Drug Dilutionthompson godfreyBelum ada peringkat
- CPV/CCV Ag (3 Lines) : VcheckDokumen2 halamanCPV/CCV Ag (3 Lines) : VcheckFoamfab WattikaBelum ada peringkat
- Obama Mind ControlDokumen68 halamanObama Mind Controlkdnkgljfg67% (3)
- Automation of Mechanical VentilationDokumen12 halamanAutomation of Mechanical VentilationjuanBelum ada peringkat
- Chapter 1Dokumen15 halamanChapter 1ErikaBelum ada peringkat
- Fetal SkullDokumen34 halamanFetal SkullNeelofur Ibran Ali85% (20)
- Chapter33Walker2015 PDFDokumen12 halamanChapter33Walker2015 PDFMai AngelBelum ada peringkat
- Radiographic EvaluationDokumen12 halamanRadiographic EvaluationLuis Gerardo Castillo MendozaBelum ada peringkat
- Safety Data Sheet: Product Name: MOBILGEAR 600 XP 320Dokumen11 halamanSafety Data Sheet: Product Name: MOBILGEAR 600 XP 320RupeshBabu SankariyaBelum ada peringkat
- Maternal and Child PreboardDokumen17 halamanMaternal and Child PreboardMichelle GambolBelum ada peringkat
- Ecg InterpretationDokumen3 halamanEcg Interpretationman0billi0% (1)
- M H Case SolutionDokumen1 halamanM H Case SolutionSai Dinesh UniqueBelum ada peringkat
- Case StudyDokumen5 halamanCase StudyHomework PingBelum ada peringkat
- Baker v. Dalkon Sheild, 156 F.3d 248, 1st Cir. (1998)Dokumen10 halamanBaker v. Dalkon Sheild, 156 F.3d 248, 1st Cir. (1998)Scribd Government DocsBelum ada peringkat
- Ross University 2010-2011 Pre-Residency Planning GuideDokumen61 halamanRoss University 2010-2011 Pre-Residency Planning GuidescatteredbrainBelum ada peringkat
- 1 s2.0 S0022391302002998 MainDokumen5 halaman1 s2.0 S0022391302002998 MainManjeev GuragainBelum ada peringkat
- Tibbonto: Knowledge Representation of Prophet Medicine (Tibb Al-Nabawi)Dokumen5 halamanTibbonto: Knowledge Representation of Prophet Medicine (Tibb Al-Nabawi)INFOPARK CSCBelum ada peringkat
- Herbal Drugs Standardization ReviewDokumen14 halamanHerbal Drugs Standardization ReviewAhmad Daud OmBelum ada peringkat
- IM Injuction: Definition of Intramuscular InjectionDokumen8 halamanIM Injuction: Definition of Intramuscular InjectiondhanasundariBelum ada peringkat
- Subfalcine Herniation Damages Cingulate GyrusDokumen34 halamanSubfalcine Herniation Damages Cingulate GyrusLorenzo FrancisBelum ada peringkat
- Staff Nurse Interview Questions 2Dokumen3 halamanStaff Nurse Interview Questions 2daciana_ilie100% (2)
- Ohi 2Dokumen6 halamanOhi 2api-242024640Belum ada peringkat
- Dreams and Disassociate CommunicationDokumen18 halamanDreams and Disassociate Communicationjeremiezulaski100% (1)
- ESB 2018 Abstract Proceedings 4Dokumen1.099 halamanESB 2018 Abstract Proceedings 4Alan PolancoBelum ada peringkat
- MRI Monitoring System Provides Safety and MobilityDokumen4 halamanMRI Monitoring System Provides Safety and MobilityAchiyat WinataBelum ada peringkat
- Firstaid ModuleDokumen143 halamanFirstaid Moduleretni wulandariBelum ada peringkat