Anda mungkin juga menyukai
- Competence Appraisal Cesarean SectionDokumen20 halamanCompetence Appraisal Cesarean SectionAnaBelum ada peringkat
- The IntegumentDokumen1 halamanThe IntegumentAnaBelum ada peringkat
- The IntegumentDokumen17 halamanThe IntegumentAnaBelum ada peringkat
- Abnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Dokumen34 halamanAbnormal Progress in Labor (Precipitous Labor and Birth & Retraction Rings)Ana100% (3)
- Beliefs and Material Culture in The PhilippinesDokumen4 halamanBeliefs and Material Culture in The PhilippinesAnaBelum ada peringkat
- Competence Appraisal Cesarean SectionDokumen20 halamanCompetence Appraisal Cesarean SectionAnaBelum ada peringkat
- Soc Sci ReportDokumen69 halamanSoc Sci ReportAnaBelum ada peringkat
- Placenta Accreta ReportDokumen13 halamanPlacenta Accreta ReportAnaBelum ada peringkat
- A Case Study On Typhoid FeverDokumen42 halamanA Case Study On Typhoid FeverAna92% (13)
- Chest PhysiotherapyDokumen5 halamanChest PhysiotherapyAnaBelum ada peringkat
- Soapie, Assessment and NCP On PAINDokumen7 halamanSoapie, Assessment and NCP On PAINAna100% (2)
- Uterine AnomaliesDokumen24 halamanUterine AnomaliesAnaBelum ada peringkat
- Assignment in NutritionDokumen12 halamanAssignment in NutritionAnaBelum ada peringkat
- Different Substance Abuse and Their Effects To Pregnancy and FetusDokumen5 halamanDifferent Substance Abuse and Their Effects To Pregnancy and FetusAnaBelum ada peringkat
- AntiPsychotic Drugs ReportDokumen56 halamanAntiPsychotic Drugs ReportAnaBelum ada peringkat
- Immune SystemDokumen58 halamanImmune SystemAnaBelum ada peringkat
- Retraction Ring LeafletDokumen2 halamanRetraction Ring LeafletAna100% (1)
- Retraction RingDokumen5 halamanRetraction RingAna100% (2)
- Prokaryotic & Eukaryotic Cells - 3Dokumen47 halamanProkaryotic & Eukaryotic Cells - 3AnaBelum ada peringkat
- CVA-Health Teaching PlanDokumen5 halamanCVA-Health Teaching PlanAna100% (4)
- FNCPDokumen9 halamanFNCPAna100% (4)
- DM-Health Teaching PlanDokumen9 halamanDM-Health Teaching PlanAna86% (7)
- Immunization SchedulesDokumen3 halamanImmunization SchedulesAnaBelum ada peringkat
- Nursery Rhyme ActivitiesDokumen13 halamanNursery Rhyme ActivitiesAnaBelum ada peringkat
- Immune System 2Dokumen39 halamanImmune System 2AnaBelum ada peringkat
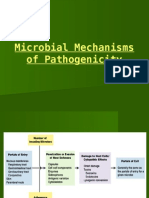
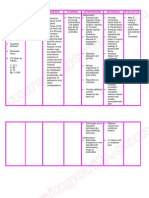
- Microbial Mechanisms of PathogenicityDokumen29 halamanMicrobial Mechanisms of PathogenicityAnaBelum ada peringkat
- Stroke (Bisaya and English)Dokumen4 halamanStroke (Bisaya and English)AnaBelum ada peringkat
- Microbial Diseases of The Skin & EyesDokumen52 halamanMicrobial Diseases of The Skin & EyesAna100% (3)
- Microbial Diseases of The Respiratory SystemDokumen9 halamanMicrobial Diseases of The Respiratory SystemAnaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Ahmed Currim's compilation of James Tyler Kent's unpublished workDokumen31 halamanAhmed Currim's compilation of James Tyler Kent's unpublished worksunnyjamiel63% (8)
- Check Your English Vocabulary For MedicineDokumen65 halamanCheck Your English Vocabulary For MedicineOlga Poleszak100% (1)
- Strategic ManagementDokumen24 halamanStrategic ManagementSonetAsrafulBelum ada peringkat
- Critical AppraisalDokumen16 halamanCritical Appraisalsigit_asoiBelum ada peringkat
- Case Report on BPH and Heart DiseaseDokumen18 halamanCase Report on BPH and Heart DiseaseAsrarudin HamidBelum ada peringkat
- Gaviscon ClinicalDokumen7 halamanGaviscon ClinicalMuhammad Nadzri NoorhayatuddinBelum ada peringkat
- Functional Crown Lengthening Surgery Periodontic and Prosthodontic ConsiderationsDokumen5 halamanFunctional Crown Lengthening Surgery Periodontic and Prosthodontic ConsiderationsNajeeb UllahBelum ada peringkat
- 2000 Sandler PJ, Atkinson R, Murray AM. For Four Sixes. Am J Orthod Dentofacial Orthop PDFDokumen17 halaman2000 Sandler PJ, Atkinson R, Murray AM. For Four Sixes. Am J Orthod Dentofacial Orthop PDFplayer osamaBelum ada peringkat
- Multiple SclerosisDokumen35 halamanMultiple SclerosisJc SeguiBelum ada peringkat
- Effects of Kinesio Taping For Stroke Patients WithDokumen8 halamanEffects of Kinesio Taping For Stroke Patients WithBias HerkawentarBelum ada peringkat
- Concept Map Epidural AbcessDokumen11 halamanConcept Map Epidural Abcessapi-593859653Belum ada peringkat
- Apollo Hospitals - First-World Health Care at Emerging - Market PricesDokumen3 halamanApollo Hospitals - First-World Health Care at Emerging - Market PricesNaveen Chander Dhar100% (1)
- Chapter 12Dokumen15 halamanChapter 12kk5522Belum ada peringkat
- Risks of Elective Cesarean SectionDokumen11 halamanRisks of Elective Cesarean SectionLutfiAnny Rahman HakimBelum ada peringkat
- MOLA's Osteology BooksDokumen1 halamanMOLA's Osteology BooksMOLA (Museum of London Archaeology)Belum ada peringkat
- 300 Video Lectures About Narcissists and PsychopathsDokumen20 halaman300 Video Lectures About Narcissists and PsychopathsSam VakninBelum ada peringkat
- Kimberly Mcneil ResumeDokumen3 halamanKimberly Mcneil ResumeKim Floyd McneilBelum ada peringkat
- Pulp Protection Methods and MaterialsDokumen13 halamanPulp Protection Methods and MaterialsmirfanulhaqBelum ada peringkat
- Effect of Aging On The ElectrocardiogramDokumen4 halamanEffect of Aging On The ElectrocardiogramHesbon MomanyiBelum ada peringkat
- AAOS Abstracts GuidelinesDokumen6 halamanAAOS Abstracts GuidelinesNuno PaisBelum ada peringkat
- Anna FreudDokumen14 halamanAnna Freudyoshita bhargavaBelum ada peringkat
- Tsr-Backpain Ebook FinalDokumen24 halamanTsr-Backpain Ebook FinalRodrigo LimaBelum ada peringkat
- Process ApproachDokumen4 halamanProcess ApproachJuan Hernández GarcíaBelum ada peringkat
- PNDFDokumen315 halamanPNDFXharisz Dulin100% (3)
- 110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFDokumen11 halaman110 TOP SURGERY Multiple Choice Questions and Answers PDF - Medical Multiple Choice Questions PDFaziz0% (1)
- Hematologic Diseases OverviewDokumen11 halamanHematologic Diseases OverviewPerrilyn Perey100% (2)
- Annotated Bibliography FormatDokumen2 halamanAnnotated Bibliography FormatJohn TerryBelum ada peringkat
- Chlamydia: Chlamydia Rapid Test Device (Swab/Urine)Dokumen3 halamanChlamydia: Chlamydia Rapid Test Device (Swab/Urine)Cristhian CuviBelum ada peringkat
- Nursing Care Plan Cesarian DeliveryDokumen2 halamanNursing Care Plan Cesarian Deliveryderic97% (39)
- Psychiatric Nursing SlidesDokumen27 halamanPsychiatric Nursing SlidesHazel RoseBelum ada peringkat