Anda mungkin juga menyukai
- Judge Aileen Cannon Grants President Trump's Request For Special Master Review of Documents Seized During Mar-a-Lago RaidDokumen24 halamanJudge Aileen Cannon Grants President Trump's Request For Special Master Review of Documents Seized During Mar-a-Lago RaidJim Hoft100% (5)
- Book - MOSBY'S DENTAL DRUG REFERENCE PDFDokumen1.496 halamanBook - MOSBY'S DENTAL DRUG REFERENCE PDFMohamed Faizal78% (9)
- Response To States 4.2 Motion in Limine Character of VictimDokumen10 halamanResponse To States 4.2 Motion in Limine Character of VictimLaw of Self DefenseBelum ada peringkat
- Sedative-Hypnotic Drugs: Michael H. Nelson, PH.D., R.PHDokumen10 halamanSedative-Hypnotic Drugs: Michael H. Nelson, PH.D., R.PHHan HopperBelum ada peringkat
- Second and Third Generation Antipsychotics: A Comprehensive HandbookDari EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookPenilaian: 5 dari 5 bintang5/5 (1)
- Students Sleep During Classes: The Amount of Time VariesDokumen7 halamanStudents Sleep During Classes: The Amount of Time Variesjason_aaBelum ada peringkat
- Oregon SOS Audit On Child WelfareDokumen49 halamanOregon SOS Audit On Child WelfareSinclair Broadcast Group - Eugene100% (1)
- Test Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDokumen3 halamanTest Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDavid Ortiz97% (36)
- Effects of GABA On Brain and BehaviourDokumen6 halamanEffects of GABA On Brain and BehaviourRay TakazaBelum ada peringkat
- Jews in Bosnia and Herzegovina PDFDokumen15 halamanJews in Bosnia and Herzegovina PDFLejla BL100% (1)
- TEACHER Healthy Diet American English Upper Intermediate Advanced GroupDokumen4 halamanTEACHER Healthy Diet American English Upper Intermediate Advanced GroupMarcus SabiniBelum ada peringkat
- FEDIAF Nutritional Guidelines 2020 20200917Dokumen96 halamanFEDIAF Nutritional Guidelines 2020 20200917luciana ribeiroBelum ada peringkat
- NCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMADokumen5 halamanNCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMAMa. Elaine Carla Tating50% (2)
- (2008) Abuse and Dependence Liability of Benzodiazepine-Type DrugsDokumen28 halaman(2008) Abuse and Dependence Liability of Benzodiazepine-Type Drugssharp8787Belum ada peringkat
- Anti Kejang Review Article BenzodiazepamDokumen18 halamanAnti Kejang Review Article Benzodiazepamgilbert defretesBelum ada peringkat
- Restoration of GABAA Receptor Function After Benzodiazepine Use - A Meta-AnalysisDokumen19 halamanRestoration of GABAA Receptor Function After Benzodiazepine Use - A Meta-AnalysisLucasBelum ada peringkat
- 2005 - GABA (A) Receptor Channel Pharmacology.Dokumen20 halaman2005 - GABA (A) Receptor Channel Pharmacology.sasaBelum ada peringkat
- 1992 M. LOEFFLER, - Oral Benzodiazepines and Conscious Sedation - A Review PAULDokumen9 halaman1992 M. LOEFFLER, - Oral Benzodiazepines and Conscious Sedation - A Review PAULAlejandro RuizBelum ada peringkat
- (1998) - Benzodiazepine Dependence From Neural Circuits To Gene Expression.Dokumen10 halaman(1998) - Benzodiazepine Dependence From Neural Circuits To Gene Expression.Aarón ParedesBelum ada peringkat
- Medicam PT InsomnDokumen13 halamanMedicam PT InsomnDoina DoniciBelum ada peringkat
- Page 1 of 16Dokumen16 halamanPage 1 of 16DNN RiadBelum ada peringkat
- Hypnotic Medications: Mechanisms of Action and Pharmacologic EffectsDokumen15 halamanHypnotic Medications: Mechanisms of Action and Pharmacologic EffectsZabb Ifha WdekhBelum ada peringkat
- ) Differential Roles of GABAA Receptor Subtypes in Benzodiazepine-Induced Enhancement of Brain-Stimulation Reward.Dokumen10 halaman) Differential Roles of GABAA Receptor Subtypes in Benzodiazepine-Induced Enhancement of Brain-Stimulation Reward.reynolds.lauBelum ada peringkat
- Drugs That Act On The CNSDokumen27 halamanDrugs That Act On The CNSnur rachmad afandiBelum ada peringkat
- PM3102 Q2Dokumen3 halamanPM3102 Q2rexlloydBelum ada peringkat
- Anxiolytic & Hypnotics Part 1Dokumen28 halamanAnxiolytic & Hypnotics Part 1Sarah ArkanBelum ada peringkat
- The Treatment of Benzodiazepine Dependence: Heather AshtonDokumen8 halamanThe Treatment of Benzodiazepine Dependence: Heather AshtonLucius MarpleBelum ada peringkat
- Bipolar Disorders and Carbamazepine PharmacokinetiDokumen6 halamanBipolar Disorders and Carbamazepine PharmacokinetiluthfiahBelum ada peringkat
- Pharm 2 TESTDokumen26 halamanPharm 2 TESTRachel MackeyBelum ada peringkat
- Gaba Receptor Modulation - To B or Not To Be B A Pro-Cognitive Medicine?Dokumen8 halamanGaba Receptor Modulation - To B or Not To Be B A Pro-Cognitive Medicine?Valeria PBelum ada peringkat
- Anti Seizure Drugs 07Dokumen27 halamanAnti Seizure Drugs 07ashokvishnoi29pBelum ada peringkat
- Anticonvulsivantes e Antipsicóticos No Tratamento Do Transtorno BipolarDokumen7 halamanAnticonvulsivantes e Antipsicóticos No Tratamento Do Transtorno BipolarAzerax PLAYBelum ada peringkat
- Ashton SupplDokumen7 halamanAshton SupplMateria TresBelum ada peringkat
- Antianxiety DrugsDokumen56 halamanAntianxiety DrugsVictor AlexandreBelum ada peringkat
- Anxiolytics and Sedative-HypnoticsDokumen27 halamanAnxiolytics and Sedative-HypnoticsLaime CaceresBelum ada peringkat
- Part I. Benzodiazepines-Side Effects, Abuse Risk and AlternativesDokumen13 halamanPart I. Benzodiazepines-Side Effects, Abuse Risk and AlternativesPamella Kusuma WerdanieBelum ada peringkat
- Rogawski Epilepsy Neurotherapeutics1996compressDokumen81 halamanRogawski Epilepsy Neurotherapeutics1996compresspentagronBelum ada peringkat
- Anti Anxiety DrugsDokumen13 halamanAnti Anxiety DrugsVamsi Krishna100% (1)
- Baclofen and Gamma-Hydroxybutyrate WithdrawalDokumen4 halamanBaclofen and Gamma-Hydroxybutyrate WithdrawalImustaforgotBelum ada peringkat
- Lacosamide: A Novel Antiepileptic and Anti-Nociceptive Drug On The BlockDokumen5 halamanLacosamide: A Novel Antiepileptic and Anti-Nociceptive Drug On The BlockFarhatBelum ada peringkat
- Gaba Is The Major Inhibitory Neurotransmitter in The Nervous SystemDokumen10 halamanGaba Is The Major Inhibitory Neurotransmitter in The Nervous SystemMount EmeraldBelum ada peringkat
- Whats Wrong With Prescribing Hipnotics?Dokumen6 halamanWhats Wrong With Prescribing Hipnotics?Alberto JaramilloBelum ada peringkat
- Gabapentin and Pregabalin For The Acute Post-Operative Pain Management. A Systematic-Narrative Review of The Recent Clinical EvidencesDokumen18 halamanGabapentin and Pregabalin For The Acute Post-Operative Pain Management. A Systematic-Narrative Review of The Recent Clinical EvidencesAndy BaiBelum ada peringkat
- Palliat Med 2004 Bennett 5 11Dokumen8 halamanPalliat Med 2004 Bennett 5 11James PerianayagamBelum ada peringkat
- Kologi 1Dokumen6 halamanKologi 1Ida BagusGede Dwi AmbaraBelum ada peringkat
- Papaer ValeDokumen8 halamanPapaer ValeDiego Alexander González CabreraBelum ada peringkat
- Treatment of Benzodiazepine DependenceDokumen8 halamanTreatment of Benzodiazepine DependenceJeffly Varro GilbertBelum ada peringkat
- GABAA Receptor Channel PharmacologyDokumen20 halamanGABAA Receptor Channel PharmacologyJuan Carlos LrBelum ada peringkat
- Benzodiazepine ReceptorsDokumen13 halamanBenzodiazepine ReceptorsjBelum ada peringkat
- Glutamate Neurotransmission in Psychotic Disorders and Substance AbuseDokumen8 halamanGlutamate Neurotransmission in Psychotic Disorders and Substance AbuseLeanne MontgomeryBelum ada peringkat
- Andrews 2018Dokumen8 halamanAndrews 2018chemistpl420Belum ada peringkat
- Med Chem NotesDokumen13 halamanMed Chem NotesPaolo PepsBelum ada peringkat
- 1 s2.0 S2667382722000096 MainDokumen14 halaman1 s2.0 S2667382722000096 MainAndrea SalazarBelum ada peringkat
- NO. 16. Ayano G (2016) Bipolar Disorders and Valproate PharmacokineticsDokumen5 halamanNO. 16. Ayano G (2016) Bipolar Disorders and Valproate PharmacokineticsVincent AriesBelum ada peringkat
- Pharmacoepidemiology of Benzodiazepine and Sedative-Hypnotic Use in A Canadian General Population Cohort During 12 Years of Follow-UpDokumen8 halamanPharmacoepidemiology of Benzodiazepine and Sedative-Hypnotic Use in A Canadian General Population Cohort During 12 Years of Follow-UpAnonymous TKSMzgRJoBBelum ada peringkat
- Mechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingDokumen4 halamanMechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingLuhur Anggoro SulistioBelum ada peringkat
- 02 Intoxicacion Benzodiacepinas PDFDokumen11 halaman02 Intoxicacion Benzodiacepinas PDFDilia Dourdane AvilaBelum ada peringkat
- For Answering Learning Issues Searching Method Inform Ation Type Validity Importance Foundatio N Result Foundatio N ResultDokumen3 halamanFor Answering Learning Issues Searching Method Inform Ation Type Validity Importance Foundatio N Result Foundatio N ResultEga Candra FaurizaBelum ada peringkat
- Anxiolytic DrugsDokumen44 halamanAnxiolytic DrugschkiershadiBelum ada peringkat
- Sedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiDokumen30 halamanSedative-Hypnotic Drugs: Department of Pharmacology Zhang YanmeiKAVITA HOODABelum ada peringkat
- A Selective Summary of Psychopharmacology Research Published in First Half of 2017Dokumen3 halamanA Selective Summary of Psychopharmacology Research Published in First Half of 2017gion.nandBelum ada peringkat
- Treatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsDokumen26 halamanTreatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsMaria Jose CastañedaBelum ada peringkat
- SedativeDokumen15 halamanSedativeManul ShobujBelum ada peringkat
- Bipolar Disorders and Carbamazepine PharmacokinetiDokumen5 halamanBipolar Disorders and Carbamazepine PharmacokinetiAgr YuroBelum ada peringkat
- Anti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreDokumen26 halamanAnti Dementia Drugs: Moderator: Dr. Ramasubbareddy Sir Presenter: Dr. RavikishoreKishore SadulaBelum ada peringkat
- Pini Lupo2001 Article Anti EpilepticDrugsInThePrevenDokumen7 halamanPini Lupo2001 Article Anti EpilepticDrugsInThePrevenPutu Gede SudiraBelum ada peringkat
- The Effects of Antiepileptic Inducers in NeuropsyDokumen7 halamanThe Effects of Antiepileptic Inducers in NeuropsyJuan IgnacioBelum ada peringkat
- (2018) Risks and Benefits of Medications For Panic Disorder A Comparison of SSRIs and BenzodiazepinesDokumen11 halaman(2018) Risks and Benefits of Medications For Panic Disorder A Comparison of SSRIs and BenzodiazepinesAarón ParedesBelum ada peringkat
- Pregabalin Hospital PharmacyDokumen16 halamanPregabalin Hospital PharmacyadityaBelum ada peringkat
- Anxiolytic DrugsDokumen60 halamanAnxiolytic Drugsneleh grayBelum ada peringkat
- Agenda and Notes For Inaugural Meeting of RAGWA Inc: Office HoldersDokumen4 halamanAgenda and Notes For Inaugural Meeting of RAGWA Inc: Office HoldersDavid KevosBelum ada peringkat
- Probolt Brochure FastenerDokumen32 halamanProbolt Brochure FastenerDavid KevosBelum ada peringkat
- Duke of Sussex V Home SecretaryDokumen11 halamanDuke of Sussex V Home SecretaryDavid KevosBelum ada peringkat
- Suspension PDFDokumen3 halamanSuspension PDFDavid KevosBelum ada peringkat
- A Review of Road Safety Governance in Western AustraliaDokumen95 halamanA Review of Road Safety Governance in Western AustraliaDavid KevosBelum ada peringkat
- DOCWA 2018 Annual ReportDokumen20 halamanDOCWA 2018 Annual ReportDavid KevosBelum ada peringkat
- Ducati 4-Valve Adjustment WorksheetDokumen5 halamanDucati 4-Valve Adjustment WorksheetDavid KevosBelum ada peringkat
- Test - K1 GSXR1000 - AMCN Vol 50 No12 22 Dec 2000Dokumen5 halamanTest - K1 GSXR1000 - AMCN Vol 50 No12 22 Dec 2000David KevosBelum ada peringkat
- Desmo Club ConstitutionDokumen34 halamanDesmo Club ConstitutionDavid KevosBelum ada peringkat
- Installation of HID Kit 848-1X98Dokumen16 halamanInstallation of HID Kit 848-1X98David KevosBelum ada peringkat
- Woollard Electorate LetterDokumen1 halamanWoollard Electorate LetterDavid KevosBelum ada peringkat
- Germany and Australia - Motorcycle Impact To Roadside BarriersDokumen13 halamanGermany and Australia - Motorcycle Impact To Roadside BarriersDavid KevosBelum ada peringkat
- DOCWA Application FormDokumen2 halamanDOCWA Application FormDavid KevosBelum ada peringkat
- Midland PT 0004Dokumen1 halamanMidland PT 0004David KevosBelum ada peringkat
- Recidivism PDFDokumen21 halamanRecidivism PDFDavid KevosBelum ada peringkat
- Repeal Carbon Tax Consultation-PaperDokumen42 halamanRepeal Carbon Tax Consultation-PaperDavid KevosBelum ada peringkat
- Inquiry Into Motorcycle Safety-ReportDokumen535 halamanInquiry Into Motorcycle Safety-ReportDavid KevosBelum ada peringkat
- Midland Reporter 231012Dokumen1 halamanMidland Reporter 231012David KevosBelum ada peringkat
- Inquiry Into Motorcycle Safety-ReportDokumen535 halamanInquiry Into Motorcycle Safety-ReportDavid KevosBelum ada peringkat
- Campbellv Woollard 2012 WADC0048Dokumen66 halamanCampbellv Woollard 2012 WADC0048David KevosBelum ada peringkat
- The Senate Proof Motions Carbon Pricing Speech: Thursday, 21 June 2012Dokumen4 halamanThe Senate Proof Motions Carbon Pricing Speech: Thursday, 21 June 2012David KevosBelum ada peringkat
- g8 Health q3 LM Disease 130908005904 PDFDokumen64 halamang8 Health q3 LM Disease 130908005904 PDFkenneth cannillBelum ada peringkat
- Adani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalDokumen20 halamanAdani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalboxorBelum ada peringkat
- Lecture in Geriatrics Physical Therapy 1Dokumen27 halamanLecture in Geriatrics Physical Therapy 1S.ABelum ada peringkat
- Providing Information Raising Awareness: June 2015Dokumen17 halamanProviding Information Raising Awareness: June 2015Aymanahmad AymanBelum ada peringkat
- NCPPDokumen11 halamanNCPPAngelo Miguel MuñozBelum ada peringkat
- Mylan EpiPen StatementDokumen3 halamanMylan EpiPen StatementCBS This MorningBelum ada peringkat
- Tcharestresumefinal 1009Dokumen2 halamanTcharestresumefinal 1009tcharestBelum ada peringkat
- MDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDDokumen8 halamanMDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDKayla GreenstienBelum ada peringkat
- MSDS Aceite CastorDokumen6 halamanMSDS Aceite CastorwaddydiBelum ada peringkat
- Professions and Occupations in BoliviaDokumen7 halamanProfessions and Occupations in BoliviaMaribel Jarata JulianBelum ada peringkat
- The Chameleon Enthusiast by Noelle SenchynaDokumen58 halamanThe Chameleon Enthusiast by Noelle SenchynaDragoș DrăniceanuBelum ada peringkat
- Coordination Group For Mutual Recognition and Decentralised Procedures - Human (CMDH)Dokumen12 halamanCoordination Group For Mutual Recognition and Decentralised Procedures - Human (CMDH)aslkdjBelum ada peringkat
- Polytechnic of Health Denpasar Is An Institution of Higher Education Official of The Department of Health Which Is The Technical Implementation UnitDokumen1 halamanPolytechnic of Health Denpasar Is An Institution of Higher Education Official of The Department of Health Which Is The Technical Implementation UnitDewi PradnyaniBelum ada peringkat
- 2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationDokumen4 halaman2016 10 12 Members Letter-HHS OCR Organ Transplant DiscriminationMike Honda100% (2)
- Acute HepatitisDokumen14 halamanAcute Hepatitisapi-379370435100% (1)
- Halamang GamotDokumen32 halamanHalamang GamotJasmin PastoresBelum ada peringkat
- PEC in INDIA ExplainationDokumen3 halamanPEC in INDIA ExplainationSaumya ChandraBelum ada peringkat
- Effects of Sprint Interval Training and Body.24Dokumen8 halamanEffects of Sprint Interval Training and Body.24Maxwell MartinsBelum ada peringkat
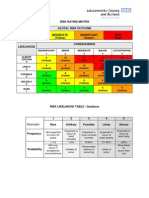
- Example of A NHS Risk Rating MatrixDokumen2 halamanExample of A NHS Risk Rating MatrixRochady SetiantoBelum ada peringkat
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDokumen2 halamanNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comBelum ada peringkat
- Assoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyDokumen8 halamanAssoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyWindyanissa RecitaBelum ada peringkat