Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- AI in Cardiovascular DiseaseDokumen11 halamanAI in Cardiovascular Diseasepartha sreekarBelum ada peringkat
- Expert Recommendations On The Assessment of Wall Shear Stress in Human Coronary ArteriesDokumen17 halamanExpert Recommendations On The Assessment of Wall Shear Stress in Human Coronary ArteriesМихаил НеболеевBelum ada peringkat
- Siemens Acuson Sc2000 Truefusion Flyer v2Dokumen4 halamanSiemens Acuson Sc2000 Truefusion Flyer v2bashir019Belum ada peringkat
- Interventional Radiology ExplainedDokumen4 halamanInterventional Radiology ExplainedAinne Joy DimapilisBelum ada peringkat
- Bachelor of Nursing Science With HonoursDokumen17 halamanBachelor of Nursing Science With HonoursMaryam HasanahBelum ada peringkat
- Austin Journal of Cardiovascular Disease and AtherosclerosisDokumen4 halamanAustin Journal of Cardiovascular Disease and AtherosclerosisAustin Publishing GroupBelum ada peringkat
- Vascular Injury Associated With Extremity Trauma .5Dokumen10 halamanVascular Injury Associated With Extremity Trauma .5Ortiz Martínez Juan GuillermoBelum ada peringkat
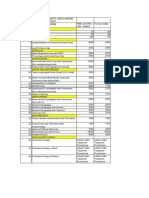
- Usulan Alat Cag Dan Pci Cathlab 2019: Nama Alat Harga Harga+Ppn Produk Jumlah KETDokumen6 halamanUsulan Alat Cag Dan Pci Cathlab 2019: Nama Alat Harga Harga+Ppn Produk Jumlah KETHaris RismantoBelum ada peringkat
- AtherosclerosisDokumen23 halamanAtherosclerosisPoonam soniBelum ada peringkat
- Log Book - 2009.ChDokumen58 halamanLog Book - 2009.ChShreyas WalvekarBelum ada peringkat
- MBF7823423Dokumen425 halamanMBF7823423Pete PetersBelum ada peringkat
- CT Angiogram Explained: How It Detects BlockagesDokumen2 halamanCT Angiogram Explained: How It Detects BlockagesfraserladsBelum ada peringkat
- Intraarterial Thrombolysis Techniques and Ongoing TrialsDokumen10 halamanIntraarterial Thrombolysis Techniques and Ongoing TrialsIustitia Septuaginta SambenBelum ada peringkat
- Case Study Ucmed 6TH FloorDokumen44 halamanCase Study Ucmed 6TH FloorPasay Trisha Faye Y.Belum ada peringkat
- Acute Mesenteric IschemiaDokumen46 halamanAcute Mesenteric Ischemiashita febrianaBelum ada peringkat
- BSC CardtechDokumen25 halamanBSC CardtechShahidriswanBelum ada peringkat
- Fundamentals of Nursing 1Dokumen6 halamanFundamentals of Nursing 1Ruel M. BersabeBelum ada peringkat
- Principles of Liver Transplantation: Types, Assessment, Timing & WorkupDokumen22 halamanPrinciples of Liver Transplantation: Types, Assessment, Timing & WorkupRajarshi KumarBelum ada peringkat
- Embolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewDokumen20 halamanEmbolization of Bronchial Arteries For The Treatment of HEMOPTYSIS. Update and Literature ReviewHai SheikhBelum ada peringkat
- Icare EIDON Family REV002 Hi ResDokumen7 halamanIcare EIDON Family REV002 Hi ResPramod UpadhyayBelum ada peringkat
- Neurosurgery Report Tuesday, January 11, 2022: Penanggung Jawab MandiriDokumen66 halamanNeurosurgery Report Tuesday, January 11, 2022: Penanggung Jawab MandiribobirfansyahputraBelum ada peringkat
- CGHS Rates TrivandrumDokumen12 halamanCGHS Rates TrivandrumarathibvaishnavBelum ada peringkat
- 1.5T MRI Systems, Issue 6. Comparative Report On Six MRI Systems.Dokumen115 halaman1.5T MRI Systems, Issue 6. Comparative Report On Six MRI Systems.Francis MannoBelum ada peringkat
- Coma and Brain DeathDokumen24 halamanComa and Brain DeathDean AccountBelum ada peringkat
- MRI and CT of The Cardiovascular SystemDokumen692 halamanMRI and CT of The Cardiovascular SystemMariluzArangoBelum ada peringkat
- In The United States District Court For The Southern District of Georgia Waycross DivisionDokumen31 halamanIn The United States District Court For The Southern District of Georgia Waycross DivisionfraudblawgBelum ada peringkat
- Head Trauma: Dr. Murk Niaz GI Surgery ResidentDokumen25 halamanHead Trauma: Dr. Murk Niaz GI Surgery ResidentMurk NiazBelum ada peringkat
- MJPJAY Procedures 996Dokumen58 halamanMJPJAY Procedures 996bhushan adhariBelum ada peringkat
- 1528PVMS Notification PART-BDokumen417 halaman1528PVMS Notification PART-BBasharatBelum ada peringkat
- Symptoms, Types and Risk Factors of StrokesDokumen12 halamanSymptoms, Types and Risk Factors of StrokesReymund Timog TalarocBelum ada peringkat