Anda mungkin juga menyukai
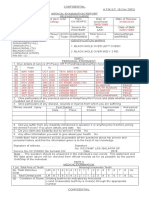
- Afms-3b (Yer 2003) AmeDokumen17 halamanAfms-3b (Yer 2003) AmeHimashree GiduguBelum ada peringkat
- Jagadees Med FormDokumen2 halamanJagadees Med FormD jagadeeswaran100% (1)
- Medical ReportDokumen2 halamanMedical ReportwildanmuhammadnajmiBelum ada peringkat
- Format Patient EncounterDokumen5 halamanFormat Patient EncounterNicholas PetrovskiBelum ada peringkat
- Medical FormDokumen4 halamanMedical FormSujata DeviBelum ada peringkat
- Critical Illness (Heart) - Statement of Medical ExaminerDokumen2 halamanCritical Illness (Heart) - Statement of Medical ExaminerUstazFaizalAriffinOriginalBelum ada peringkat
- Borang Pemeriksaan KesihatanDokumen4 halamanBorang Pemeriksaan KesihatanMan DenzoBelum ada peringkat
- TYPED-medical SoftDokumen5 halamanTYPED-medical SoftynrajambaBelum ada peringkat
- Physical Fitness CertificateDokumen1 halamanPhysical Fitness CertificateDilip SenthBelum ada peringkat
- SaftyDokumen3 halamanSaftyAnonymous ABLtDDvKuiBelum ada peringkat
- Medical Board 210122Dokumen6 halamanMedical Board 210122Holi PanBelum ada peringkat
- HKCAD Medical Report FormDokumen4 halamanHKCAD Medical Report FormHelloWorldBelum ada peringkat
- 1 Medical Board Format ESE 091216Dokumen6 halaman1 Medical Board Format ESE 091216ryy38480Belum ada peringkat
- Form4 COPDokumen3 halamanForm4 COPAdarsh RaghuwanshiBelum ada peringkat
- Docs To Be SubmittedDokumen15 halamanDocs To Be Submittedgourkanti213Belum ada peringkat
- Asuhan Keperawatan Di Instalasi Gawat DaruratDokumen5 halamanAsuhan Keperawatan Di Instalasi Gawat DaruratAnnaBelum ada peringkat
- Asuhan Keperawatan Di Instalasi Gawat DaruratDokumen5 halamanAsuhan Keperawatan Di Instalasi Gawat DaruratrisaBelum ada peringkat
- Asuhan Keperawatan Di Instalasi Gawat DaruratDokumen5 halamanAsuhan Keperawatan Di Instalasi Gawat DaruratRidha TiomantaBelum ada peringkat
- Asuhan Keperawatan Di Instalasi Gawat DaruratDokumen5 halamanAsuhan Keperawatan Di Instalasi Gawat DaruratDyah PerwaBelum ada peringkat
- Asuhan Keperawatan Di Instalasi Gawat DaruratDokumen5 halamanAsuhan Keperawatan Di Instalasi Gawat DaruratLatifah khusnul SugiartoBelum ada peringkat
- Proforma Age Estimation PDFDokumen3 halamanProforma Age Estimation PDFYogitaBelum ada peringkat
- Annual Medical/Special Medical Examinations Performa For CRPF Personnel: NgosDokumen3 halamanAnnual Medical/Special Medical Examinations Performa For CRPF Personnel: NgosTowards HappinessBelum ada peringkat
- Physical Fitness CertificateDokumen2 halamanPhysical Fitness CertificateRavi Kiran BBelum ada peringkat
- Food Handlers Medical FormDokumen1 halamanFood Handlers Medical FormAnnu Rajesh100% (2)
- Medical Examination - FormDokumen3 halamanMedical Examination - FormVivek KumarBelum ada peringkat
- Medical Examination Form NewDokumen2 halamanMedical Examination Form NewShady SharmaBelum ada peringkat
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2)Dokumen2 halamanIcmr Specimen Referral Form For Covid-19 (Sars-Cov2)Divin MatthewBelum ada peringkat
- Medical Board Format 2015Dokumen6 halamanMedical Board Format 2015hemantaduttaghy1Belum ada peringkat
- Form 44Dokumen3 halamanForm 44Aditya AryaBelum ada peringkat
- Shekhawati Form - FDokumen2 halamanShekhawati Form - FArchit ChampanekarBelum ada peringkat
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDokumen4 halamanConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaBelum ada peringkat
- Form Blood RequisitionDokumen2 halamanForm Blood Requisitionshubham kumar ram100% (1)
- 3.medical FormDokumen5 halaman3.medical Formamistudio30Belum ada peringkat
- Monitoring Format - 18072023Dokumen5 halamanMonitoring Format - 18072023IT AAMC CellBelum ada peringkat
- Maritime Declaration of Health: Note: Please Consult "Fields Description" Sheet Before Filling The FieldsDokumen16 halamanMaritime Declaration of Health: Note: Please Consult "Fields Description" Sheet Before Filling The Fieldsenciu georgeBelum ada peringkat
- Maritime Declaration of Health Mesaieed and Ras Laffan PortDokumen2 halamanMaritime Declaration of Health Mesaieed and Ras Laffan PortOleksii SolomakhaBelum ada peringkat
- Maritime Declaration of HealthDokumen1 halamanMaritime Declaration of Healthalive2flirt100% (1)
- MedicalDokumen2 halamanMedicalOseghale MichaelBelum ada peringkat
- 3DCA-CUIAB-C79254 - ARB-07/22/2016-Appellant Reply BriefDokumen56 halaman3DCA-CUIAB-C79254 - ARB-07/22/2016-Appellant Reply BriefJerry VashchookBelum ada peringkat
- Medical Certificate FormDokumen1 halamanMedical Certificate FormDEEPAKBelum ada peringkat
- Maritime DeclarationDokumen1 halamanMaritime DeclarationGogiBelum ada peringkat
- Medical Examiner'S Confidential ReportDokumen2 halamanMedical Examiner'S Confidential ReportParesh BorboruahBelum ada peringkat
- Model of Maritime Declaration of Health: Annex 8Dokumen1 halamanModel of Maritime Declaration of Health: Annex 8Dian Pratiwi AkbarBelum ada peringkat
- Model Maritime Declaration of HealthDokumen2 halamanModel Maritime Declaration of Healthrpg154Belum ada peringkat
- Form O New FormatDokumen3 halamanForm O New FormatGaurav Jangid100% (1)
- Assesment Neonate 2Dokumen9 halamanAssesment Neonate 2vivien kate perixBelum ada peringkat
- Lome Model Maritime Declaration of HealthDokumen2 halamanLome Model Maritime Declaration of HealthObaroBelum ada peringkat
- O-PEL003 Application For Issue or Renewal of CPLDokumen2 halamanO-PEL003 Application For Issue or Renewal of CPLibromed16Belum ada peringkat
- Ant Is One of Small Animal Included Into Family FormicidaeDokumen3 halamanAnt Is One of Small Animal Included Into Family FormicidaeUjang SyafirinBelum ada peringkat
- Certificate of HealthDokumen2 halamanCertificate of HealthmohamedydBelum ada peringkat
- L 2. A-L/9 3. Satisfactory? A-L/9? A-L/9? Test 6. Duties? 7. Fitness?Dokumen2 halamanL 2. A-L/9 3. Satisfactory? A-L/9? A-L/9? Test 6. Duties? 7. Fitness?Zyan TahsanBelum ada peringkat
- Accused ProformaDokumen7 halamanAccused ProformaYogitaBelum ada peringkat
- Health Fitness Certificate For The Purposes of Permission To Work in Confined SpaceDokumen6 halamanHealth Fitness Certificate For The Purposes of Permission To Work in Confined SpaceNur ShaBelum ada peringkat
- Schedule of Events-1Dokumen3 halamanSchedule of Events-1Sri RhishiBelum ada peringkat
- Maritime Health DeclarationDokumen1 halamanMaritime Health DeclarationRAUNAK KUMARBelum ada peringkat
- Maritime Declaration of HealthDokumen2 halamanMaritime Declaration of Health황교민Belum ada peringkat
- Form SOLI Z PolskiDokumen3 halamanForm SOLI Z Polskiabdelhamid chakriBelum ada peringkat
- FORM 1 (Registration)Dokumen4 halamanFORM 1 (Registration)Suraj PathakBelum ada peringkat
- 1425 Question PaperDokumen2 halaman1425 Question PaperPacific TigerBelum ada peringkat
- Material CostDokumen23 halamanMaterial CostPacific TigerBelum ada peringkat
- 806 Question PaperDokumen1 halaman806 Question PaperPacific TigerBelum ada peringkat
- 4725 Question PaperDokumen2 halaman4725 Question PaperPacific TigerBelum ada peringkat
- 548 Question PaperDokumen3 halaman548 Question PaperPacific TigerBelum ada peringkat
- 943 Question PaperDokumen2 halaman943 Question PaperPacific TigerBelum ada peringkat
- 25 Question PaperDokumen4 halaman25 Question PaperPacific TigerBelum ada peringkat
- 25 Question PaperDokumen4 halaman25 Question PaperPacific Tiger0% (1)
- Labour CostDokumen8 halamanLabour CostPacific TigerBelum ada peringkat
- 3903 Question PaperDokumen2 halaman3903 Question PaperPacific TigerBelum ada peringkat
- 3300 Question PaperDokumen2 halaman3300 Question PaperPacific TigerBelum ada peringkat
- 3300 Question PaperDokumen4 halaman3300 Question PaperPacific TigerBelum ada peringkat
- 3903 Question PaperDokumen4 halaman3903 Question PaperPacific TigerBelum ada peringkat
- 1044 Question PaperDokumen2 halaman1044 Question PaperPacific TigerBelum ada peringkat
- 943 Question PaperDokumen3 halaman943 Question PaperPacific TigerBelum ada peringkat
- 63 Question PaperDokumen2 halaman63 Question PaperPacific TigerBelum ada peringkat
- 553 Question PaperDokumen2 halaman553 Question PaperPacific TigerBelum ada peringkat
- 152 Question PaperDokumen2 halaman152 Question PaperPacific TigerBelum ada peringkat
- Presentation On Bio Concrete BY Kabilan.MDokumen16 halamanPresentation On Bio Concrete BY Kabilan.MPacific TigerBelum ada peringkat
- 427 Question PaperDokumen2 halaman427 Question PaperPacific TigerBelum ada peringkat
- HR Management ThesisDokumen82 halamanHR Management Thesismithun_antony100% (1)
- Theory Exam On Operating System mm:100Dokumen1 halamanTheory Exam On Operating System mm:100Pacific TigerBelum ada peringkat
- Presentation On Bio Concrete BY Kabilan.MDokumen16 halamanPresentation On Bio Concrete BY Kabilan.MPacific TigerBelum ada peringkat
- 250 Question PaperDokumen2 halaman250 Question PaperPacific TigerBelum ada peringkat
- 25 Question PaperDokumen4 halaman25 Question PaperPacific TigerBelum ada peringkat
- Numbers For ComplaintsDokumen14 halamanNumbers For ComplaintsPacific TigerBelum ada peringkat
- Arti (Erp)Dokumen1 halamanArti (Erp)Pacific TigerBelum ada peringkat
- Study On Self-Healing Concrete Types - A Review: Ishraq Mohammad Ali Khattab, Hazhar Shekha, Mohammed Abukar AbdiDokumen12 halamanStudy On Self-Healing Concrete Types - A Review: Ishraq Mohammad Ali Khattab, Hazhar Shekha, Mohammed Abukar AbdiPacific TigerBelum ada peringkat
- 08 Jul 2023 Manipal LabReportDokumen3 halaman08 Jul 2023 Manipal LabReportMUKUL JANGIDBelum ada peringkat
- Draft Loa 03-2021 - OkDokumen5 halamanDraft Loa 03-2021 - OkTrần Thanh ViệnBelum ada peringkat
- Lipid ChemDokumen6 halamanLipid ChemKarla Faye UcangBelum ada peringkat
- Nutrition For Life: Fat: An Essential Energy-Supplying NutrientDokumen23 halamanNutrition For Life: Fat: An Essential Energy-Supplying Nutrientjuiceman222Belum ada peringkat
- Test Report: Hemogram Test Name Units Results Bio. Ref. IntervalDokumen19 halamanTest Report: Hemogram Test Name Units Results Bio. Ref. Intervalcs2015ok77Belum ada peringkat
- Types of FatDokumen3 halamanTypes of FatDennis Mark PalimaBelum ada peringkat
- Lipid MetabolismDokumen9 halamanLipid MetabolismDianaMamaligaBelum ada peringkat
- Chlosteral LPTestDokumen4 halamanChlosteral LPTestJohn StupBelum ada peringkat
- STA 399 Free Glycerol Assay Kit FluorometricDokumen6 halamanSTA 399 Free Glycerol Assay Kit FluorometricAHMADI TORKAMANI, MAHSA (조형예술대학 디자인학부) Belum ada peringkat
- Stoker Chapter19 (Lipids) - 2 PDFDokumen85 halamanStoker Chapter19 (Lipids) - 2 PDFAsther Mantua86% (7)
- Quiz Lipids and LipoproteinsDokumen9 halamanQuiz Lipids and LipoproteinsAllyah Ross DuqueBelum ada peringkat
- Bio ,, OSPEDokumen10 halamanBio ,, OSPEOsama BakheetBelum ada peringkat
- Lecture: Structure and Functions of LipidsDokumen7 halamanLecture: Structure and Functions of LipidslaceyBelum ada peringkat
- HiperkolesterolDokumen60 halamanHiperkolesterolAnonymous 1jCVqQuBelum ada peringkat
- Proceedings T H E Nutrition Society: Triglyceride Fats I N Human Nutrition F.R.S.Dokumen8 halamanProceedings T H E Nutrition Society: Triglyceride Fats I N Human Nutrition F.R.S.Akshita SabharwalBelum ada peringkat
- LipoproteinsDokumen30 halamanLipoproteinsApurba PradhanBelum ada peringkat
- CHIMICA PANZIERI Industrial-CatalogueDokumen28 halamanCHIMICA PANZIERI Industrial-CatalogueJose E BatistaBelum ada peringkat
- JURNALDokumen9 halamanJURNALAnnisa HasanahBelum ada peringkat
- Nr. Crt. CNP Lipide COL LDL HDL TG Mediu (R/U) Imagist Ica: Arges 05/18/2021 Pg. 1/10Dokumen10 halamanNr. Crt. CNP Lipide COL LDL HDL TG Mediu (R/U) Imagist Ica: Arges 05/18/2021 Pg. 1/10marinescu danBelum ada peringkat
- Reagen EKatalog 2019Dokumen10 halamanReagen EKatalog 2019erwin januarBelum ada peringkat
- Waxes and SteroidsDokumen7 halamanWaxes and SteroidsAllyssa FernandezBelum ada peringkat
- The Lipids What Are Lipids?Dokumen16 halamanThe Lipids What Are Lipids?Sire100% (1)
- Pharmacotherapy of Dyslipidemia by DR SarmaDokumen123 halamanPharmacotherapy of Dyslipidemia by DR Sarmamae2003Belum ada peringkat
- 11 05 Lipids PDFDokumen5 halaman11 05 Lipids PDFSweta SumanBelum ada peringkat
- Lec. 12 Biochemistry IIDokumen22 halamanLec. 12 Biochemistry IIGames beautifulBelum ada peringkat
- Determination of Serum LipidsDokumen2 halamanDetermination of Serum LipidsKabo Wale100% (2)
- (WORKSHEET) General Biology 1 2nd Quarter Activity 2 - LipidsDokumen2 halaman(WORKSHEET) General Biology 1 2nd Quarter Activity 2 - Lipidsaltheatoledo15Belum ada peringkat
- Saturated and Unsaturated FatsDokumen5 halamanSaturated and Unsaturated FatsKhor Z ShanBelum ada peringkat
- Jivo Canola Oil - Jivo Wellness PVT LTD ProfileDokumen10 halamanJivo Canola Oil - Jivo Wellness PVT LTD ProfileRps KohliBelum ada peringkat
- FATS AND OTHER LIPIDS Report Basic Nutri Group 5 BSND1ADokumen19 halamanFATS AND OTHER LIPIDS Report Basic Nutri Group 5 BSND1AMA. NECOLE JEREMIAH GONZALESBelum ada peringkat