Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- GI BleedDokumen96 halamanGI Bleedjaish8904100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Population Dynamics and Control of ContraceptionDokumen16 halamanPopulation Dynamics and Control of Contraceptionjaish8904Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Medical Assessment Qs 20160501Dokumen10 halamanMedical Assessment Qs 20160501jaish8904Belum ada peringkat
- Blood Grouping (BCS) LDokumen10 halamanBlood Grouping (BCS) Ljaish8904Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- PitcDokumen12 halamanPitcjaish8904Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- HORMONAL CONTRACEPTION PresentationDokumen25 halamanHORMONAL CONTRACEPTION Presentationjaish8904Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Histology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana UniversityDokumen39 halamanHistology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana Universityjaish8904Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- 4) Crude, Specific and Adjusted RateDokumen19 halaman4) Crude, Specific and Adjusted Ratejaish8904100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Name: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal InfluenzaDokumen13 halamanName: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal Influenzajaish8904Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Management of InfluenzaDokumen14 halamanManagement of Influenzajaish8904Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Lecture Wirawan Ing Desk Cross Sectional 2009Dokumen22 halamanLecture Wirawan Ing Desk Cross Sectional 2009jaish8904Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Care Support TreatmentDokumen10 halamanCare Support Treatmentjaish8904Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- 3) Measurement of Mortality and MorbidityDokumen21 halaman3) Measurement of Mortality and Morbidityjaish8904100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Cohort 1Dokumen25 halamanCohort 1jaish8904Belum ada peringkat
- Neonatal Nutrition: Mohammad KhassawnehDokumen34 halamanNeonatal Nutrition: Mohammad Khassawnehjaish8904Belum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Kuliah Blok Growth and DevelopmentDokumen44 halamanKuliah Blok Growth and Developmentjaish8904Belum ada peringkat
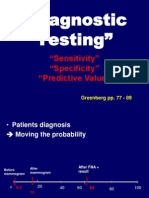
- "Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"Dokumen11 halaman"Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"jaish8904Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Conse LingDokumen39 halamanConse Lingjaish8904Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- NCP - Anxiety and DepressionDokumen2 halamanNCP - Anxiety and DepressionJenny Agustin FabrosBelum ada peringkat
- Major Depressive Disorder: Presented By: Justin Darrell A. SALACUPDokumen15 halamanMajor Depressive Disorder: Presented By: Justin Darrell A. SALACUPJoana Mikee Rasay100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Pangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanDokumen8 halamanPangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanferdzBelum ada peringkat
- 4682 VKCBCXBBDokumen40 halaman4682 VKCBCXBBمحمد عقيليBelum ada peringkat
- First Step To Achieve Your Objective - GomezDokumen8 halamanFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoBelum ada peringkat
- HEAD AND SPINAL INJURY - DR RetnoDokumen22 halamanHEAD AND SPINAL INJURY - DR RetnoJackBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Seizure Disorders and Management in Primary Health CareDokumen83 halamanSeizure Disorders and Management in Primary Health CareChidi MbatuegwuBelum ada peringkat
- Long-Acting Injectable Antipsychotics Shall The Last Be First 2014Dokumen3 halamanLong-Acting Injectable Antipsychotics Shall The Last Be First 2014Fan TomasBelum ada peringkat
- Phase 2 ActiveLearningTemplate SysDisDokumen2 halamanPhase 2 ActiveLearningTemplate SysDisFelixBelum ada peringkat
- NAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Dokumen9 halamanNAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Shreekrishna BudhathokiBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Brain TumorsDokumen3 halamanBrain TumorsDrashty DesaiBelum ada peringkat
- Understand The Facts - Anxiety and Depression Association of America, ADAADokumen5 halamanUnderstand The Facts - Anxiety and Depression Association of America, ADAAAhmad Badius ZamanBelum ada peringkat
- A Presentation On: by K.Chaitanya (MAPC)Dokumen24 halamanA Presentation On: by K.Chaitanya (MAPC)NishthaBelum ada peringkat
- Q.P. Code: 641375Dokumen7 halamanQ.P. Code: 641375Mani RuzzamanBelum ada peringkat
- IPSCPGSUDSynopsisBook2015 PDFDokumen130 halamanIPSCPGSUDSynopsisBook2015 PDFSarbartha PramanikBelum ada peringkat
- System Disorder: PneumothoraxDokumen1 halamanSystem Disorder: PneumothoraxEli ReyesBelum ada peringkat
- Lesson 4 - Electrolyte Imbalances Part 1Dokumen74 halamanLesson 4 - Electrolyte Imbalances Part 1Clark SavageBelum ada peringkat
- A Case of A Young Man With Severe HypertensiDokumen4 halamanA Case of A Young Man With Severe HypertensiProject dronacharyapwBelum ada peringkat
- Primary Survey AssessmentDokumen52 halamanPrimary Survey Assessmentlapkas donjuanBelum ada peringkat
- APA - DSM5 - Severity Measure For Social Anxiety Disorder Adult PDFDokumen3 halamanAPA - DSM5 - Severity Measure For Social Anxiety Disorder Adult PDFMelissandreBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Gait DisordersDokumen43 halamanGait Disordersmendato marcabanBelum ada peringkat
- Neebs Mental Health Nursing 5th Edition Ebook PDFDokumen61 halamanNeebs Mental Health Nursing 5th Edition Ebook PDFdavid.drew550100% (42)
- Goldman-Cecil Medicine 26th Edition 2020 (Dragged)Dokumen14 halamanGoldman-Cecil Medicine 26th Edition 2020 (Dragged)rpascua123100% (1)
- Guillain Barre SyndromeDokumen16 halamanGuillain Barre SyndromeNeha Rathore100% (1)
- Development in Down SyndromeDokumen30 halamanDevelopment in Down SyndromeRoilan MarlangBelum ada peringkat
- Pregnancy Induced HypertensionDokumen4 halamanPregnancy Induced HypertensionFatmah Sarah CornellBelum ada peringkat
- Icd-10 & 9 Irm RSB WSDokumen4 halamanIcd-10 & 9 Irm RSB WSArya WiradewaBelum ada peringkat
- Obstructed LabourDokumen10 halamanObstructed LabourAfra AshiqueBelum ada peringkat
- DrChris 8:17 CIO ReportDokumen14 halamanDrChris 8:17 CIO ReportDr Paul PerkoulidisBelum ada peringkat
- Fall Risk Assessment - HomecareDokumen1 halamanFall Risk Assessment - HomecareanumolBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- The Stoic Mindset: Living the Ten Principles of StoicismDari EverandThe Stoic Mindset: Living the Ten Principles of StoicismPenilaian: 4.5 dari 5 bintang4.5/5 (11)