Anda mungkin juga menyukai
- 0-00035Dokumen8 halaman0-00035Aldebaran Osuna ChaidezBelum ada peringkat
- IndianJAnaesth555463-5853193 161531Dokumen7 halamanIndianJAnaesth555463-5853193 161531Aldebaran Osuna ChaidezBelum ada peringkat
- Identify and Treat Underlying Cause: Persistent Tachyarrhythmia CausingDokumen1 halamanIdentify and Treat Underlying Cause: Persistent Tachyarrhythmia CausingLeigh DaltonBelum ada peringkat
- Series VistasDokumen4 halamanSeries VistasAldebaran Osuna ChaidezBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Clopidogrel Plus Aspirin Versus Aspirn Alone For Acute Minor Ischaemic Stroke or High Risk TIA. BMJ Dec 2018Dokumen10 halamanClopidogrel Plus Aspirin Versus Aspirn Alone For Acute Minor Ischaemic Stroke or High Risk TIA. BMJ Dec 2018oussama dieselBelum ada peringkat
- A To Z Orthodontics Vol 24 Orthodontic Practical NotesDokumen83 halamanA To Z Orthodontics Vol 24 Orthodontic Practical Notesdent in dentist100% (2)
- Eye Exercises For Healthy Eye: September 2015Dokumen3 halamanEye Exercises For Healthy Eye: September 2015spiridon_andrei2011Belum ada peringkat
- Alliance in Couple and Family TherapyDokumen10 halamanAlliance in Couple and Family TherapylpandradevBelum ada peringkat
- 52 Mutatie Brca Si Adn TerapieDokumen9 halaman52 Mutatie Brca Si Adn TerapieGabriela MilitaruBelum ada peringkat
- Principii Psiho OncologieDokumen16 halamanPrincipii Psiho OncologieCristina Tulba100% (1)
- PsychiatryDokumen18 halamanPsychiatryCarlos HernándezBelum ada peringkat
- Fractional CO2 Laser Effective for Treating OnychomycosisDokumen8 halamanFractional CO2 Laser Effective for Treating OnychomycosismyztBelum ada peringkat
- Nursing Process Mcqs Session by Husain.ZDokumen14 halamanNursing Process Mcqs Session by Husain.ZInam ullah KhanBelum ada peringkat
- Discipline of CounsellingDokumen16 halamanDiscipline of CounsellingJeffrey de LeonBelum ada peringkat
- Duty Report: Eye Clinic Case StudiesDokumen43 halamanDuty Report: Eye Clinic Case StudiesriskhapangestikaBelum ada peringkat
- Introduction To Clinical AssessmentDokumen13 halamanIntroduction To Clinical AssessmentnurmeenBelum ada peringkat
- Banana - Recommendations For Maintaining Postharvest Quality - Postharvest Technology Center - UC Davis PDFDokumen3 halamanBanana - Recommendations For Maintaining Postharvest Quality - Postharvest Technology Center - UC Davis PDFFernando SanchezBelum ada peringkat
- (Research Paper) KaushalDokumen7 halaman(Research Paper) KaushalKaushal PatelBelum ada peringkat
- Pranic HealingDokumen26 halamanPranic HealingMuhammad Hasnain Zahid100% (5)
- Soil AnalysisDokumen12 halamanSoil AnalysisSunit Hazarika100% (1)
- Pomegranate One Fruit That Cures Hundred AilmentsDokumen8 halamanPomegranate One Fruit That Cures Hundred AilmentsAsad ImranBelum ada peringkat
- Ot ProtocolDokumen38 halamanOt ProtocolSelva KumarBelum ada peringkat
- Intramuscular CKLDokumen2 halamanIntramuscular CKLapi-310181843Belum ada peringkat
- Operating TheaterDokumen5 halamanOperating Theateraksinu100% (1)
- AARC Clinical Practice Guideline: Static Lung Volumes: 2001 Revision & UpdateDokumen9 halamanAARC Clinical Practice Guideline: Static Lung Volumes: 2001 Revision & UpdateFarhana Fefe Amani FeFeBelum ada peringkat
- IBRA Scholarship Report Dr. Martin CzinnerDokumen3 halamanIBRA Scholarship Report Dr. Martin Czinnerseng li chewBelum ada peringkat
- Advanced Pathophysiology of COPD, Pulmonary Embolism and Respiratory FailureDokumen1 halamanAdvanced Pathophysiology of COPD, Pulmonary Embolism and Respiratory FailureTeanu Jose Gabrillo TamayoBelum ada peringkat
- Safety Data SheetDokumen7 halamanSafety Data SheettienBelum ada peringkat
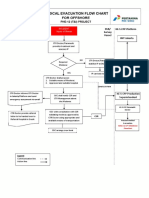
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Dokumen1 halaman3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaBelum ada peringkat
- Chapter 4 - P4 P5 The Role of Complementary TherapiesDokumen8 halamanChapter 4 - P4 P5 The Role of Complementary TherapiesdesbestBelum ada peringkat
- Fpsyt 13 1049476Dokumen12 halamanFpsyt 13 1049476putriBelum ada peringkat
- Complicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorDokumen35 halamanComplicatii Si Sechele Tardive Dupa Tratamentul Multimodal Al GlioamelorBiblioteca CSNTBelum ada peringkat
- Chinese Pastoral Counselling Course SyllabusDokumen13 halamanChinese Pastoral Counselling Course SyllabusAbinayaBelum ada peringkat
- Bio OssDokumen4 halamanBio OssVizi AdrianBelum ada peringkat