Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Room: - Name: - Code Status: - AllergiesDokumen2 halamanRoom: - Name: - Code Status: - Allergiesashdmb217Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- HCP FormDokumen8 halamanHCP FormMarkBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Brain 3Dokumen3 halamanBrain 3Nurse Betty100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Room: - Name: - Code Status: - AllergiesDokumen2 halamanRoom: - Name: - Code Status: - Allergiesashdmb217Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Starting Out - New in The ICUDokumen30 halamanStarting Out - New in The ICUashdmb217100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Useful Spanish Words and PhrasesDokumen32 halamanUseful Spanish Words and Phrasesashdmb217Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Student Clinical Report SheetDokumen2 halamanStudent Clinical Report SheetMike100% (4)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Clinical Experience "Tips"Dokumen5 halamanClinical Experience "Tips"ashdmb217Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Maxwell Quick Medical Reference PDFDokumen35 halamanMaxwell Quick Medical Reference PDFAnonymous fj68Ms100% (10)
- SymbolsDokumen1 halamanSymbolsashdmb217Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Adventitious Breath SoundsDokumen1 halamanAdventitious Breath Soundsashdmb217Belum ada peringkat
- Critical Care PhysiologyDokumen287 halamanCritical Care Physiologyashdmb217100% (7)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Nurse Brain Sheet Telemetry Unit SBARDokumen1 halamanNurse Brain Sheet Telemetry Unit SBARashdmb217Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Nursing Management of The Perioperative PatientDokumen16 halamanNursing Management of The Perioperative Patientashdmb217Belum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Medical TerminologyDokumen13 halamanMedical Terminologyashdmb217Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Information Regarding Family History DocumentDokumen9 halamanInformation Regarding Family History Documentashdmb217Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Histology Exam 2 Review.1Dokumen18 halamanHistology Exam 2 Review.1ashdmb217Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Iron regulation and water-soluble vitamin functionsDokumen3 halamanIron regulation and water-soluble vitamin functionsashdmb217Belum ada peringkat
- Histology Exam 3 ReviewDokumen7 halamanHistology Exam 3 Reviewashdmb217Belum ada peringkat
- Histology Exam IV Review Part 2Dokumen26 halamanHistology Exam IV Review Part 2ashdmb217Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- AbbreviationsDokumen5 halamanAbbreviationsashdmb217Belum ada peringkat
- Nutrition Review1.2Dokumen12 halamanNutrition Review1.2ashdmb217Belum ada peringkat
- Histology Exam IV Review Part 1Dokumen36 halamanHistology Exam IV Review Part 1ashdmb217Belum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
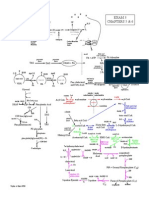
- Exam 3 PathwaysDokumen1 halamanExam 3 Pathwaysashdmb217Belum ada peringkat
- Exam IV ReviewDokumen39 halamanExam IV Reviewashdmb217Belum ada peringkat
- Exam 4 PathwaysDokumen1 halamanExam 4 Pathwaysashdmb217Belum ada peringkat
- Exam 1 Study Guide.2Dokumen52 halamanExam 1 Study Guide.2ashdmb217Belum ada peringkat
- Biochem Exam 2 Review.2Dokumen31 halamanBiochem Exam 2 Review.2ashdmb217Belum ada peringkat
- Biochem Exam III Review.2Dokumen24 halamanBiochem Exam III Review.2ashdmb217Belum ada peringkat
- Social Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictDokumen3 halamanSocial Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictRashmi MishraBelum ada peringkat
- Remembering Abram Hoffer SsDokumen104 halamanRemembering Abram Hoffer SsSchool Vegetable Gardening100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Lipid Lowering AgentsDokumen2 halamanLipid Lowering Agentsapi-623203696Belum ada peringkat
- Biochemistry - Nutrition - Module 5 60 Random Questions For MCQ TestDokumen4 halamanBiochemistry - Nutrition - Module 5 60 Random Questions For MCQ Testkirki pBelum ada peringkat
- Tiens Product Guide PDFDokumen36 halamanTiens Product Guide PDFKweku Robertson100% (1)
- Hyperlipidemia Guide: Causes, Symptoms and TreatmentDokumen17 halamanHyperlipidemia Guide: Causes, Symptoms and Treatmentbent alfay7a2Belum ada peringkat
- Turmeric Nutrition FactsDokumen40 halamanTurmeric Nutrition FactsUdhaya KumarBelum ada peringkat
- Adrenochrome Hypothesis and PsychiatryDokumen14 halamanAdrenochrome Hypothesis and PsychiatryErik KammlerBelum ada peringkat
- Successful Treatment of Schizophrenia Requires Optimal Daily Doses of Vitamin b3Dokumen5 halamanSuccessful Treatment of Schizophrenia Requires Optimal Daily Doses of Vitamin b3Joop WezenbeekBelum ada peringkat
- Nutrition Plays An Important Role in Improving The Growth and Development of SilkwormDokumen25 halamanNutrition Plays An Important Role in Improving The Growth and Development of SilkwormNarasimha Murthy0% (1)
- AbramHoffer Orthomolecular Psychiatry What Would Abram Hoffer Do 29.2Dokumen13 halamanAbramHoffer Orthomolecular Psychiatry What Would Abram Hoffer Do 29.2Ebook PDF100% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Niacine (Vitamin B3) PDFDokumen12 halamanNiacine (Vitamin B3) PDFGuranda SilvianBelum ada peringkat
- Nutrition Quiz Tests Food Group KnowledgeDokumen11 halamanNutrition Quiz Tests Food Group KnowledgePearl Aude100% (9)
- Bitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemDokumen34 halamanBitterness Compounds in Coffee Brew Measured by Analytical Instruments and Taste Sensing SystemSolisBelum ada peringkat
- Vitamin B ComplexDokumen32 halamanVitamin B ComplexAlain J. GagnonBelum ada peringkat
- International Society of Sports Nutrition Position Stand Energy Drinks and Energy ShotsDokumen73 halamanInternational Society of Sports Nutrition Position Stand Energy Drinks and Energy ShotsCarlos RamírezBelum ada peringkat
- Enzyme Catalysis-Chapter 7 (Part 1)Dokumen22 halamanEnzyme Catalysis-Chapter 7 (Part 1)OmSilence2651Belum ada peringkat
- Nutrient Requirements of Indian Major Carp: Protein and Amino AcidsDokumen4 halamanNutrient Requirements of Indian Major Carp: Protein and Amino AcidsBadrul HassanBelum ada peringkat
- MSc Home Economics Food & Nutrition MCQsDokumen153 halamanMSc Home Economics Food & Nutrition MCQsSaba ChaudhryBelum ada peringkat
- Sources of Different Vitamins and Diseases Caused by Their DeficiencyDokumen2 halamanSources of Different Vitamins and Diseases Caused by Their DeficiencyPrashant SuryawanshiBelum ada peringkat
- Milk Calcium Dietary Supplement 600 MG 100 Soft GelsDokumen3 halamanMilk Calcium Dietary Supplement 600 MG 100 Soft Gelssindi setiyadiBelum ada peringkat
- Chemical Compositions of Ipomea Aquatica Green Kangkong PDFDokumen7 halamanChemical Compositions of Ipomea Aquatica Green Kangkong PDFPaul DizonBelum ada peringkat
- 27 - Najla - Tugas Individu PSGDokumen7 halaman27 - Najla - Tugas Individu PSGDIII - Gizi - NajlaBelum ada peringkat
- Burning Feet SyndromeDokumen4 halamanBurning Feet SyndromeSellappan MuthusamyBelum ada peringkat
- Biology Form 4 Chapter 6 - VitaminsDokumen3 halamanBiology Form 4 Chapter 6 - VitaminsSim Zong Xern0% (1)
- Water-soluble Vitamins CompilationDokumen5 halamanWater-soluble Vitamins CompilationJustin AncogBelum ada peringkat
- University of The Philippines ManilaDokumen11 halamanUniversity of The Philippines ManilaAngeli Jean Koreen CorpuzBelum ada peringkat
- Food Chemistry Lecture on VitaminsDokumen50 halamanFood Chemistry Lecture on VitaminsQamber pkBelum ada peringkat
- Niacinamide and The SkinDokumen6 halamanNiacinamide and The SkinLesti LubisBelum ada peringkat
- Fortified Rice Kernel Manufacturing Industry: (Capacity: 200kgs Per Hour)Dokumen57 halamanFortified Rice Kernel Manufacturing Industry: (Capacity: 200kgs Per Hour)charsaubees420Belum ada peringkat
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossDari EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossPenilaian: 4 dari 5 bintang4/5 (22)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDari EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisPenilaian: 3 dari 5 bintang3/5 (2)
- Forever Strong: A New, Science-Based Strategy for Aging WellDari EverandForever Strong: A New, Science-Based Strategy for Aging WellBelum ada peringkat
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanDari EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthDari EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthBelum ada peringkat
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthDari EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthPenilaian: 5 dari 5 bintang5/5 (37)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDari EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyPenilaian: 5 dari 5 bintang5/5 (1)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainDari EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainPenilaian: 3.5 dari 5 bintang3.5/5 (6)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeDari EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifePenilaian: 5 dari 5 bintang5/5 (1)